Anda mungkin juga menyukai
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesDari EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesPenilaian: 4 dari 5 bintang4/5 (2)
- Lentiglp-1 Injection Decreased Blood Glucose Levels of Obese Diabetic SDW RatsDokumen1 halamanLentiglp-1 Injection Decreased Blood Glucose Levels of Obese Diabetic SDW RatsAytuğ AksakalBelum ada peringkat
- Role of Leptin in The Regulation of Glucagon-LikeDokumen8 halamanRole of Leptin in The Regulation of Glucagon-Likea12345644321Belum ada peringkat
- Prof. Yaron Ilan - Glycosphingolipids Improve Glucose Intolerance and Hepatic Steatosis of The Cohen Diabetic RatDokumen7 halamanProf. Yaron Ilan - Glycosphingolipids Improve Glucose Intolerance and Hepatic Steatosis of The Cohen Diabetic RatProf. Yaron IlanBelum ada peringkat
- Coppari 2012. Bases Molecular de La Resistencia A La LeptinaDokumen17 halamanCoppari 2012. Bases Molecular de La Resistencia A La LeptinaClaudioValdiviaBelum ada peringkat
- Adiponectin Leptin and Leptin Receptor in Obese PaDokumen15 halamanAdiponectin Leptin and Leptin Receptor in Obese PaDZGR NNBelum ada peringkat
- Effect of Insulin Analog Initiation Therapy On LDL/ HDL Subfraction Profile and HDL Associated Enzymes in Type 2 Diabetic PatientsDokumen11 halamanEffect of Insulin Analog Initiation Therapy On LDL/ HDL Subfraction Profile and HDL Associated Enzymes in Type 2 Diabetic PatientsAan AlawiyahBelum ada peringkat
- Case 2Dokumen23 halamanCase 2EJ CorpusBelum ada peringkat
- Chronic Effect of PferospermuDokumen1 halamanChronic Effect of PferospermuamritaryaaligarghBelum ada peringkat
- Regulation of Lipogenesis by Glucocorticoids and Insulin in Human Adipose TissueDokumen9 halamanRegulation of Lipogenesis by Glucocorticoids and Insulin in Human Adipose TissuemamithemadBelum ada peringkat
- Hbo in The Metabolic Control of Insulin-Dependent Diabetes Mellitus: A Controlled StudyDokumen6 halamanHbo in The Metabolic Control of Insulin-Dependent Diabetes Mellitus: A Controlled StudyThumiso MasohaBelum ada peringkat
- GLP-1 Elicits An Intrinsic Gut-Liver Metabolic Signal To Ameliorate Diet-Induced VLDL Overproduction and Insulin ResistanceDokumen8 halamanGLP-1 Elicits An Intrinsic Gut-Liver Metabolic Signal To Ameliorate Diet-Induced VLDL Overproduction and Insulin ResistanceAnditri WeningtyasBelum ada peringkat
- Insulin 2 PDFDokumen15 halamanInsulin 2 PDFAnonymous K9tmd7T0PzBelum ada peringkat
- Recent Advances in Incretin-Based Pharmacotherapies For The Treatment of Obesity and DiabetesDokumen3 halamanRecent Advances in Incretin-Based Pharmacotherapies For The Treatment of Obesity and DiabetesAndrés ChávezBelum ada peringkat
- Transcriptomic and Proteomic Analysis of Potential Therapeutic Target Genes in The Liver of Metformin Treated Sprague Dawley Rats With Type 2 Diabetes Mellitusijmm-41!06!3327Dokumen15 halamanTranscriptomic and Proteomic Analysis of Potential Therapeutic Target Genes in The Liver of Metformin Treated Sprague Dawley Rats With Type 2 Diabetes Mellitusijmm-41!06!3327ErickBelum ada peringkat
- Adiponectin: Chien-Wen Chou MD. Endocrinology & Metabolism Division Chi-Mei Medical Center 22 April 2005Dokumen18 halamanAdiponectin: Chien-Wen Chou MD. Endocrinology & Metabolism Division Chi-Mei Medical Center 22 April 2005Efi RamadhaniBelum ada peringkat
- Combination Treatment With Insulin and Oral Agents in Type 2 Diabetes MellitusDokumen6 halamanCombination Treatment With Insulin and Oral Agents in Type 2 Diabetes MellitusEstiPramestiningtyasBelum ada peringkat
- Changes in Insulin Resistance Following BariatricDokumen8 halamanChanges in Insulin Resistance Following Bariatrica12345644321Belum ada peringkat
- Berberine Moderates Glucose and Lipid Metabolism TDokumen10 halamanBerberine Moderates Glucose and Lipid Metabolism THitesh VermaBelum ada peringkat
- Characteristic of GLP-1 Effects On Glucose Metabolism in Human Skeletal Muscle From Obese PatientsDokumen6 halamanCharacteristic of GLP-1 Effects On Glucose Metabolism in Human Skeletal Muscle From Obese PatientsfrandellionBelum ada peringkat
- Administration of An Acylated GLP-1 and GIP Preparation Provides Added Beneficial Glucose-Lowering and Insulinotropic Actions Over Single Incretins in Mice With Type 2 Diabetes and ObesityDokumen11 halamanAdministration of An Acylated GLP-1 and GIP Preparation Provides Added Beneficial Glucose-Lowering and Insulinotropic Actions Over Single Incretins in Mice With Type 2 Diabetes and ObesitypdgcssBelum ada peringkat
- Liver So RosDokumen5 halamanLiver So RosAnnette CraigBelum ada peringkat
- Physiology of Glucose Homeostasis and Insulin Therapy in Type 1 and Type 2 Diabetes (2012)Dokumen15 halamanPhysiology of Glucose Homeostasis and Insulin Therapy in Type 1 and Type 2 Diabetes (2012)drheayBelum ada peringkat
- Clinical Review 124 Diabetic Dyslipidemia: Causes and ConsequencesDokumen7 halamanClinical Review 124 Diabetic Dyslipidemia: Causes and ConsequencesjessicaBelum ada peringkat
- Inhibition of Carbohydrate-Mediated Glucagon-Like Peptide-1 (7-36) Amide Secretion by Circulating Non-Esterified Fatty AcidsDokumen8 halamanInhibition of Carbohydrate-Mediated Glucagon-Like Peptide-1 (7-36) Amide Secretion by Circulating Non-Esterified Fatty AcidsRidha Surya NugrahaBelum ada peringkat
- Fisiologi of PankreasDokumen9 halamanFisiologi of PankreasSunardi BahriBelum ada peringkat
- Grupo 3 Obesity InflammationDokumen9 halamanGrupo 3 Obesity InflammationJeisonAlejandroÁlvarezVergaraBelum ada peringkat
- Zhou 2019Dokumen11 halamanZhou 2019Andreea Claudia NegrilaBelum ada peringkat
- Reduced Postprandial Concentrations of Intact Biologically Active Glucagon-Like Peptide 1 in Type 2 Diabetic PatientsDokumen5 halamanReduced Postprandial Concentrations of Intact Biologically Active Glucagon-Like Peptide 1 in Type 2 Diabetic PatientsRoger CBelum ada peringkat
- Chapter 60Dokumen7 halamanChapter 60Ridha Surya NugrahaBelum ada peringkat
- Resolving The Paradox of Hepatic Insulin ResistanceDokumen10 halamanResolving The Paradox of Hepatic Insulin ResistanceMauro Rojas ZúñigaBelum ada peringkat
- Tutor: Prof. DR. Yasmin Amr.: Subject: CHO and Lipid MetabolismDokumen8 halamanTutor: Prof. DR. Yasmin Amr.: Subject: CHO and Lipid MetabolismHashim OmarBelum ada peringkat
- Mietlickibaase 2017Dokumen31 halamanMietlickibaase 2017Isa AguilarBelum ada peringkat
- 29126.1 20150227101459 CoveredDokumen10 halaman29126.1 20150227101459 CoveredeeeeBelum ada peringkat
- Cellular Mechanism of DM FinalDokumen70 halamanCellular Mechanism of DM FinalJamil Muqtadir BhattiBelum ada peringkat
- Biology 09 00473 v3Dokumen20 halamanBiology 09 00473 v3Gaby CarellanoBelum ada peringkat
- Protective Effects of GLP-1 On Glomerular Endothelium and Its Inhibition by PKC Activation in DiabetesDokumen14 halamanProtective Effects of GLP-1 On Glomerular Endothelium and Its Inhibition by PKC Activation in DiabetesRidha Surya NugrahaBelum ada peringkat
- Downsi 6 PDFDokumen11 halamanDownsi 6 PDFmutimutimutiBelum ada peringkat
- 19 10835Dokumen7 halaman19 10835LiaaBelum ada peringkat
- The Integrative Biology of Type 2 DiabetesDokumen10 halamanThe Integrative Biology of Type 2 DiabetesAdrian GhiţăBelum ada peringkat
- Incretin PharmDokumen3 halamanIncretin PharmSlim SaaryBelum ada peringkat
- Jurnal Interna (Penyakit Usus)Dokumen7 halamanJurnal Interna (Penyakit Usus)BayuptrBelum ada peringkat
- 764 FullDokumen6 halaman764 FullRidha Surya NugrahaBelum ada peringkat
- 2015 Article 45Dokumen9 halaman2015 Article 45Dr. Kaushal Kishor SharmaBelum ada peringkat
- Dipeptidyl Peptidase (DPP) - IV InhibitorDokumen2 halamanDipeptidyl Peptidase (DPP) - IV InhibitorAndhi FahrurrojiBelum ada peringkat
- Lipoprotein Metabolism in Patients With Type 1 Diabetes Under Intensive Insulin TreatmentDokumen10 halamanLipoprotein Metabolism in Patients With Type 1 Diabetes Under Intensive Insulin TreatmentayuwdystBelum ada peringkat
- Tirzepatide Versus Semaglutide Once Weekly in Patients With Type 2 DiabetesDokumen13 halamanTirzepatide Versus Semaglutide Once Weekly in Patients With Type 2 Diabetesmanish chaudharyBelum ada peringkat
- Is GLP-1 A Hormone: Whether and When?: David D 'AlessioDokumen6 halamanIs GLP-1 A Hormone: Whether and When?: David D 'AlessioGaby NRmzBelum ada peringkat
- Diet Induced Dyslipidemia Leads To Nonalcoholic Fatty Live 2016 TranslationaDokumen15 halamanDiet Induced Dyslipidemia Leads To Nonalcoholic Fatty Live 2016 TranslationaRafaelaBelum ada peringkat
- Selected AbstractsDokumen3 halamanSelected AbstractsJaime Muñoz FrancoBelum ada peringkat
- Sugary Kefir Strain Lactobacillus Mali APS1 Ameliorated Hepatic Steatosis by Regulation of SIRT-1 NR-2 and Gut Microbiota in RatsDokumen24 halamanSugary Kefir Strain Lactobacillus Mali APS1 Ameliorated Hepatic Steatosis by Regulation of SIRT-1 NR-2 and Gut Microbiota in RatsCristina OliveiraBelum ada peringkat
- Perspectives: G Protein-Coupled Receptors As Targets For Anti-Diabetic TherapeuticsDokumen13 halamanPerspectives: G Protein-Coupled Receptors As Targets For Anti-Diabetic TherapeuticsAlicia Cerpa LunaBelum ada peringkat
- Momordica Charantia Scientific Paper 6Dokumen1 halamanMomordica Charantia Scientific Paper 6arjunismeBelum ada peringkat
- Improvement in Glycemia After Glucose or Insulin Overload in Leptin-Infused Rats Is Associated With Insulin-Related Activation of Hepatic Glucose MetabolismDokumen6 halamanImprovement in Glycemia After Glucose or Insulin Overload in Leptin-Infused Rats Is Associated With Insulin-Related Activation of Hepatic Glucose MetabolismDaniel Gomez GalindoBelum ada peringkat
- Advanced PathophysiologyDokumen23 halamanAdvanced PathophysiologyNijaya MohantoBelum ada peringkat
- Glucagon-Like Peptide 1: New: TherapiesDokumen3 halamanGlucagon-Like Peptide 1: New: TherapiesRidha Surya NugrahaBelum ada peringkat
- Administration of Resveratrol For 5 WK Has No Effect On Glucagon-Like Peptide 1 Secretion, Gastric Emptying, or Glycemic Control in Type 2 Diabetes: A Randomized Controlled TrialDokumen5 halamanAdministration of Resveratrol For 5 WK Has No Effect On Glucagon-Like Peptide 1 Secretion, Gastric Emptying, or Glycemic Control in Type 2 Diabetes: A Randomized Controlled TrialAmanda TeacaBelum ada peringkat
- HFD MiceDokumen5 halamanHFD Micechar462Belum ada peringkat
- Peptides: John P. Gleeson, Joanne Heade, Sinéad M. Ryan, David J. BraydenDokumen7 halamanPeptides: John P. Gleeson, Joanne Heade, Sinéad M. Ryan, David J. Braydensuci apsari pebriantiBelum ada peringkat
- Article-2012-Vaspin in Obesity and Diabetes-Pathophysiological and Clinical SignificanceDokumen7 halamanArticle-2012-Vaspin in Obesity and Diabetes-Pathophysiological and Clinical Significancecarlos ArozamenaBelum ada peringkat
- Direct X EulaDokumen2 halamanDirect X EulaApriPutra95Belum ada peringkat
- Common FilelistDokumen1 halamanCommon Filelistluisgerardo000000Belum ada peringkat
- FitoquimiaDokumen2 halamanFitoquimialuisgerardo000000Belum ada peringkat
- HE Genomic Basis OF Trophic Strategy IN Marine BacteriaDokumen17 halamanHE Genomic Basis OF Trophic Strategy IN Marine Bacterialuisgerardo000000Belum ada peringkat
- Int Workbook 3Dokumen92 halamanInt Workbook 3rcam3717050% (2)
- Presented byDokumen9 halamanPresented byeshikaBelum ada peringkat
- Dietary Reference IntakeDokumen7 halamanDietary Reference IntakePolene AfableBelum ada peringkat
- Discharge PlanDokumen2 halamanDischarge Plan2G Balatayo Joshua LeoBelum ada peringkat
- Medical Surgical Challenge and Practice TestDokumen12 halamanMedical Surgical Challenge and Practice TestLim Eric100% (1)
- Remission of Type 2 Diabetes. Canada TF 2022Dokumen13 halamanRemission of Type 2 Diabetes. Canada TF 2022DrasmBelum ada peringkat
- Introduction To Food Science Edited 15. 09.2019Dokumen37 halamanIntroduction To Food Science Edited 15. 09.2019Jessica chi100% (1)
- BenfotiamineDokumen5 halamanBenfotiaminekether.thipharet5601Belum ada peringkat
- The Cornflake DietDokumen8 halamanThe Cornflake DietSorindah MolinaBelum ada peringkat
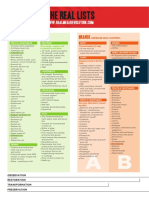
- Real Meal RevolutionTHE-LIST-A4Dokumen2 halamanReal Meal RevolutionTHE-LIST-A4fridayschild2012Belum ada peringkat
- 100 Workouts 2015Dokumen209 halaman100 Workouts 2015Diana RiosBelum ada peringkat
- Mohammad Ali LeghariDokumen64 halamanMohammad Ali LeghariNaoBelum ada peringkat
- Orange Peel Feasibility StudyDokumen82 halamanOrange Peel Feasibility StudyrotajessicabsaBelum ada peringkat
- Full Body Kettle BallDokumen1 halamanFull Body Kettle BallMario RendonBelum ada peringkat
- Chemistry Project Report On Food AdulterationDokumen9 halamanChemistry Project Report On Food AdulterationSweetha PrakashBelum ada peringkat
- TDEE Variant With BF 3.06Dokumen10 halamanTDEE Variant With BF 3.06Collette PetitBelum ada peringkat
- Tabla Alimentos NepalDokumen86 halamanTabla Alimentos NepalcarolinaBelum ada peringkat
- Experiment No. 10 - Fermented Green MangoesDokumen2 halamanExperiment No. 10 - Fermented Green MangoesMary Rose CatalbasBelum ada peringkat
- E-1 ZUIV MagazineDokumen16 halamanE-1 ZUIV MagazineSelaseh Pashur AkahoBelum ada peringkat
- Uasa Year 4Dokumen9 halamanUasa Year 4Miko Miki100% (1)
- Evidence-Based Practice Project: Diabetes Diet Management: Stephanie Green NUR - 590Dokumen20 halamanEvidence-Based Practice Project: Diabetes Diet Management: Stephanie Green NUR - 590dennis ndegeBelum ada peringkat
- Men's Health Magazine UK Issue 2017Dokumen217 halamanMen's Health Magazine UK Issue 2017Night100% (1)
- Mapeh 10 Q4 M6Dokumen31 halamanMapeh 10 Q4 M6Lore Isabel Mendoza PaclebBelum ada peringkat
- Nutritional AssessmentDokumen5 halamanNutritional AssessmentimnasBelum ada peringkat
- The 5 Tibetan Rites Is An Ancient Exercise System From TibetDokumen16 halamanThe 5 Tibetan Rites Is An Ancient Exercise System From TibetMadalina SoldanBelum ada peringkat
- Body MechanicsDokumen2 halamanBody MechanicsKarLo TabuzoBelum ada peringkat
- Project Task: Context and Conditions of AssessmentDokumen15 halamanProject Task: Context and Conditions of AssessmentSUKH100% (1)
- Food Production Yield ManagementDokumen3 halamanFood Production Yield ManagementArghajoti DeyBelum ada peringkat
- Tai Sophia Institute Whole Foods Cooking Lab 4 Nutrition 684 Fall 2012 .5 Credits FacultyDokumen5 halamanTai Sophia Institute Whole Foods Cooking Lab 4 Nutrition 684 Fall 2012 .5 Credits Facultyapi-96990759Belum ada peringkat
- Edible Landscaping PDFDokumen3 halamanEdible Landscaping PDFManu MandaBelum ada peringkat
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsDari EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsPenilaian: 5 dari 5 bintang5/5 (97)
- Relentless: From Good to Great to UnstoppableDari EverandRelentless: From Good to Great to UnstoppablePenilaian: 5 dari 5 bintang5/5 (788)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouDari EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouPenilaian: 3.5 dari 5 bintang3.5/5 (5)
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerDari EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerPenilaian: 4 dari 5 bintang4/5 (5)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayDari EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayBelum ada peringkat
- Pranayama: The Yoga Science of BreathingDari EverandPranayama: The Yoga Science of BreathingPenilaian: 4.5 dari 5 bintang4.5/5 (8)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindDari EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindPenilaian: 4.5 dari 5 bintang4.5/5 (1)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceDari EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformancePenilaian: 4.5 dari 5 bintang4.5/5 (237)
- The Total Kettlebell Workout: Trade Secrets of a Personal TrainerDari EverandThe Total Kettlebell Workout: Trade Secrets of a Personal TrainerPenilaian: 5 dari 5 bintang5/5 (1)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionDari EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionPenilaian: 3.5 dari 5 bintang3.5/5 (11)
- The Yogi Code: Seven Universal Laws of Infinite SuccessDari EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (104)
- True Yoga: Practicing With the Yoga Sutras for Happiness & Spiritual FulfillmentDari EverandTrue Yoga: Practicing With the Yoga Sutras for Happiness & Spiritual FulfillmentPenilaian: 4.5 dari 5 bintang4.5/5 (22)
- The Power of Fastercise: Using the New Science of Signaling Exercise to Get Surprisingly Fit in Just a Few Minutes a DayDari EverandThe Power of Fastercise: Using the New Science of Signaling Exercise to Get Surprisingly Fit in Just a Few Minutes a DayPenilaian: 4 dari 5 bintang4/5 (4)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!Dari EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Penilaian: 4.5 dari 5 bintang4.5/5 (22)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingDari EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingPenilaian: 4.5 dari 5 bintang4.5/5 (67)
- Strength Training Over 40: The Only Weight Training Workout Book You Will Need to Maintain or Build Your Strength, Muscle Mass, Energy, Overall Fitness and Stay Healthy Without Living in the GymDari EverandStrength Training Over 40: The Only Weight Training Workout Book You Will Need to Maintain or Build Your Strength, Muscle Mass, Energy, Overall Fitness and Stay Healthy Without Living in the GymPenilaian: 4 dari 5 bintang4/5 (6)
- Mind Your Body: 4 Weeks to a Leaner, Healthier LifeDari EverandMind Your Body: 4 Weeks to a Leaner, Healthier LifePenilaian: 4.5 dari 5 bintang4.5/5 (5)
- Enter The Kettlebell!: Strength Secret of the Soviet SupermenDari EverandEnter The Kettlebell!: Strength Secret of the Soviet SupermenPenilaian: 4 dari 5 bintang4/5 (29)
- Easy Strength: How to Get a Lot Stronger Than Your Competition-And Dominate in Your SportDari EverandEasy Strength: How to Get a Lot Stronger Than Your Competition-And Dominate in Your SportPenilaian: 4.5 dari 5 bintang4.5/5 (17)
- Tibetan Yoga: Magical Movements of Body, Breath, and MindDari EverandTibetan Yoga: Magical Movements of Body, Breath, and MindPenilaian: 5 dari 5 bintang5/5 (1)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.Dari EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Penilaian: 4.5 dari 5 bintang4.5/5 (124)
- Fascia: A Comprehensive Guide to Fascia Stretch Training (Explain the Effects on the Body Due to the Connection)Dari EverandFascia: A Comprehensive Guide to Fascia Stretch Training (Explain the Effects on the Body Due to the Connection)Belum ada peringkat
- Roxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingDari EverandRoxane Gay & Everand Originals: Built for This: The Quiet Strength of PowerliftingPenilaian: 4.5 dari 5 bintang4.5/5 (133)
- Calisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesDari EverandCalisthenics: Guide for Bodyweight Exercise, Build your Dream Body in 30 MinutesPenilaian: 3 dari 5 bintang3/5 (5)
- Wheels of Life: A User's Guide to the Chakra SystemDari EverandWheels of Life: A User's Guide to the Chakra SystemPenilaian: 4.5 dari 5 bintang4.5/5 (34)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeDari EverandYamas & Niyamas: Exploring Yoga's Ethical PracticePenilaian: 4.5 dari 5 bintang4.5/5 (111)
- The Science of Getting Ripped: Proven Diet Hacks and Workout Tricks to Burn Fat and Build Muscle in Half the TimeDari EverandThe Science of Getting Ripped: Proven Diet Hacks and Workout Tricks to Burn Fat and Build Muscle in Half the TimePenilaian: 4 dari 5 bintang4/5 (8)