Anda mungkin juga menyukai
- Employability Skills of Higher Education Graduates: Little Consensus On A Much-Discussed SubjectDokumen6 halamanEmployability Skills of Higher Education Graduates: Little Consensus On A Much-Discussed SubjectjeevanetBelum ada peringkat
- Gramin Dak Sevak Results for TamilnaduDokumen138 halamanGramin Dak Sevak Results for TamilnadumegalaBelum ada peringkat
- Dimensions of Employability Skills: Redeemer's University Journal of Management and Social Sciences June 2017Dokumen8 halamanDimensions of Employability Skills: Redeemer's University Journal of Management and Social Sciences June 2017jeevanetBelum ada peringkat
- Aim:To Create An Interactive Animation Using Maya Animation SoftwareDokumen13 halamanAim:To Create An Interactive Animation Using Maya Animation SoftwarejeevanetBelum ada peringkat
- History (Important 5 Marks)Dokumen3 halamanHistory (Important 5 Marks)jeevanetBelum ada peringkat
- History (Important 5 Marks)Dokumen3 halamanHistory (Important 5 Marks)jeevanetBelum ada peringkat
- Caring The Least of Mankind (CLM) TrustDokumen1 halamanCaring The Least of Mankind (CLM) TrustjeevanetBelum ada peringkat
- Resume for Receptionist and Sales AccountantDokumen2 halamanResume for Receptionist and Sales AccountantjeevanetBelum ada peringkat
- Mineral, Forest and Agro-based Micro EnterprisesDokumen10 halamanMineral, Forest and Agro-based Micro EnterprisesjeevanetBelum ada peringkat
- 10th April 2014 MathematicsDokumen12 halaman10th April 2014 MathematicsjeevanetBelum ada peringkat
- 1 s2.0 S1877050917325711 MainDokumen8 halaman1 s2.0 S1877050917325711 MainjeevanetBelum ada peringkat
- Technical Assistant Electrical PDFDokumen1.227 halamanTechnical Assistant Electrical PDFjeevanetBelum ada peringkat
- Employability Skills of Higher Education Graduates: Little Consensus On A Much-Discussed SubjectDokumen6 halamanEmployability Skills of Higher Education Graduates: Little Consensus On A Much-Discussed SubjectjeevanetBelum ada peringkat
- Employability Skills PDFDokumen9 halamanEmployability Skills PDFjeevanetBelum ada peringkat
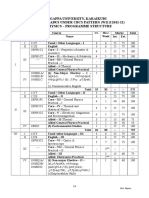
- B.SC., Physics 2011-12Dokumen30 halamanB.SC., Physics 2011-12jeevanetBelum ada peringkat
- Challenges Facing Women Employees in IndiaDokumen3 halamanChallenges Facing Women Employees in IndiajeevanetBelum ada peringkat
- M.phil Application RegulationDokumen7 halamanM.phil Application RegulationjeevanetBelum ada peringkat
- Chapter 2Dokumen24 halamanChapter 2jeevanetBelum ada peringkat
- PH.D Pre-Entrance ApplicationDokumen4 halamanPH.D Pre-Entrance ApplicationjeevanetBelum ada peringkat
- 673 1928 1 PB PDFDokumen6 halaman673 1928 1 PB PDFjeevanetBelum ada peringkat
- Mathematics IIIDokumen4 halamanMathematics IIIjeevanetBelum ada peringkat
- T.S. No.211-2014-15 PDFDokumen9 halamanT.S. No.211-2014-15 PDFjeevanetBelum ada peringkat
- Full ProjectDokumen66 halamanFull ProjectjeevanetBelum ada peringkat
- BD - Ipr133219 - Tender Form English Namakkal, Kovilpatti and Vellore 2016 PDFDokumen8 halamanBD - Ipr133219 - Tender Form English Namakkal, Kovilpatti and Vellore 2016 PDFjeevanetBelum ada peringkat
- Boq 19594Dokumen3 halamanBoq 19594jeevanetBelum ada peringkat
- Laratta WP10Dokumen14 halamanLaratta WP10jeevanetBelum ada peringkat
- S.No Content Page - NoDokumen1 halamanS.No Content Page - NojeevanetBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- JUDUL LTA 2019 OkDokumen55 halamanJUDUL LTA 2019 Oksyifa istiqomahBelum ada peringkat
- Brauchle - Ethics Scholarly Paper - Nur 335Dokumen12 halamanBrauchle - Ethics Scholarly Paper - Nur 335api-405374041Belum ada peringkat
- CV Updated 3/21Dokumen5 halamanCV Updated 3/21Abbey FritschBelum ada peringkat
- LMMC ManagementDokumen44 halamanLMMC ManagementLuciano LaranjeiraBelum ada peringkat
- Materi Binus Career Semester Genap 2022 P1Dokumen31 halamanMateri Binus Career Semester Genap 2022 P1perencanaan m2uBelum ada peringkat
- Assessment of The Awareness, Perception, Attitudes, and Preparedness of Health-Care Professionals Potentially Exposed To COVID-19 in The United Arab EmiratesDokumen12 halamanAssessment of The Awareness, Perception, Attitudes, and Preparedness of Health-Care Professionals Potentially Exposed To COVID-19 in The United Arab EmiratesSarah SanadBelum ada peringkat
- NCM18: Care of The Clients With Life Threatening Conditions: Please Answer The Following QuestionsDokumen2 halamanNCM18: Care of The Clients With Life Threatening Conditions: Please Answer The Following Questionserjen gamingBelum ada peringkat
- Checklist PULSE RATE.V2Dokumen1 halamanChecklist PULSE RATE.V2chanise casemBelum ada peringkat
- Opinion On Construction in Times of PandemicDokumen2 halamanOpinion On Construction in Times of PandemicLizeth MorenoBelum ada peringkat
- Caring-A-Patient-With-A-CastDokumen1 halamanCaring-A-Patient-With-A-CastMac Cristian A. CaraganBelum ada peringkat
- BCCH PRAM Score For Assessment For AsthmaDokumen3 halamanBCCH PRAM Score For Assessment For Asthmadini kusmaharaniBelum ada peringkat
- NIPER Library Journal Subscriptions ListDokumen4 halamanNIPER Library Journal Subscriptions ListdrugdrugBelum ada peringkat
- North Maine POS Ancillary ProfessionalsDokumen202 halamanNorth Maine POS Ancillary ProfessionalsMaine Trust For Local NewsBelum ada peringkat
- 1587-Article Text-4297-2-10-20200712Dokumen9 halaman1587-Article Text-4297-2-10-20200712Susi SusantiBelum ada peringkat
- Legal Nurse Consultant Litigation in NYC NY CT NJ Resume Sally Ann CullenDokumen2 halamanLegal Nurse Consultant Litigation in NYC NY CT NJ Resume Sally Ann CullenSallyAnnCullenBelum ada peringkat
- How To Start Your Herbal CareerDokumen100 halamanHow To Start Your Herbal Careeradrians3852100% (4)
- Designed, Tested and Trusted by Operating Theatre ProfessionalsDokumen5 halamanDesigned, Tested and Trusted by Operating Theatre ProfessionalsYusuf Selim ErkenBelum ada peringkat
- Art in Occupational TherapyDokumen10 halamanArt in Occupational TherapyGiselle Pezoa WattsonBelum ada peringkat
- Textbook Survey Results 201102Dokumen102 halamanTextbook Survey Results 201102tokionas100% (1)
- My Nursing PhilosophyDokumen5 halamanMy Nursing Philosophyapi-376802969Belum ada peringkat
- Nursing Informatics Sample Quiz 2 Multiple ChoiceDokumen2 halamanNursing Informatics Sample Quiz 2 Multiple ChoicejanmalexxBelum ada peringkat
- Che 262 Referral System and Outreach ServicesDokumen15 halamanChe 262 Referral System and Outreach ServicesBalkos 61100% (3)
- Geriatric Health Care Team Week 5Dokumen26 halamanGeriatric Health Care Team Week 5Vin SageBelum ada peringkat
- Medication OrderDokumen16 halamanMedication OrderAnonymous whcvnPBeQBelum ada peringkat
- Computer Assisted Instruction For Patient EducationDokumen9 halamanComputer Assisted Instruction For Patient EducationCorrine IvyBelum ada peringkat
- Intensive Nursing PracticumDokumen16 halamanIntensive Nursing PracticumSanjie Eufracio100% (3)
- Gmail Bachelor of Occupational Therapy (Honours)Dokumen2 halamanGmail Bachelor of Occupational Therapy (Honours)Mr NaserBelum ada peringkat
- EMDR Therapy: A 40-Character Title for PTSD TreatmentDokumen11 halamanEMDR Therapy: A 40-Character Title for PTSD TreatmentHassanBelum ada peringkat
- Periodontal Chart Dan Periodontal Risk AssessmentDokumen8 halamanPeriodontal Chart Dan Periodontal Risk AssessmentIndah VitasariBelum ada peringkat
- Counseling Competencies and SpecializationsDokumen3 halamanCounseling Competencies and SpecializationsAc Janery MamacBelum ada peringkat