Anda mungkin juga menyukai
- Renal TraumaDokumen53 halamanRenal TraumaPhilipus Putra RaharjoBelum ada peringkat
- There Are Two Types of Nociceptors Corresponding ToDokumen6 halamanThere Are Two Types of Nociceptors Corresponding ToPhilipus Putra RaharjoBelum ada peringkat
- Ondansentron in Diarrhea PDFDokumen8 halamanOndansentron in Diarrhea PDFPhilipus Putra RaharjoBelum ada peringkat
- ARIA Report 2008Dokumen196 halamanARIA Report 2008jasbroBelum ada peringkat
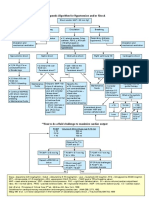
- Therapeutic Algorithm For HypotensionDokumen1 halamanTherapeutic Algorithm For HypotensionPhilipus Putra RaharjoBelum ada peringkat
- Drug-Body Interactions & PharmacokineticsDokumen9 halamanDrug-Body Interactions & PharmacokineticsPhilipus Putra RaharjoBelum ada peringkat
- AKI ChinaDokumen7 halamanAKI ChinaPhilipus Putra RaharjoBelum ada peringkat
- Acute Kidney Injury - Final Version (08 March 2011)Dokumen59 halamanAcute Kidney Injury - Final Version (08 March 2011)Abdel-hafiz MamounBelum ada peringkat
- Mcgraw-Hill: Deep Pain From Visceral and Skeletomuscular Structures IsDokumen2 halamanMcgraw-Hill: Deep Pain From Visceral and Skeletomuscular Structures IsPhilipus Putra RaharjoBelum ada peringkat
- Propionic AcidemiaDokumen4 halamanPropionic AcidemiaPhilipus Putra RaharjoBelum ada peringkat
- Moles and Skin LesionsDokumen5 halamanMoles and Skin LesionsPhilipus Putra RaharjoBelum ada peringkat
- The Primary Survey: Cervical Spine Management Chapter 1.12Dokumen5 halamanThe Primary Survey: Cervical Spine Management Chapter 1.12Philipus Putra RaharjoBelum ada peringkat
- McKinley Health CenterDokumen4 halamanMcKinley Health CenterPhilipus Putra RaharjoBelum ada peringkat
- Jet LagDokumen7 halamanJet LagPhilipus Putra RaharjoBelum ada peringkat
- Leukemia - Topic OverviewDokumen5 halamanLeukemia - Topic OverviewPhilipus Putra RaharjoBelum ada peringkat
- At A Glace MedicineDokumen365 halamanAt A Glace MedicinePhilipus Putra RaharjoBelum ada peringkat
- Digital MedicineDokumen223 halamanDigital MedicinePhilipus Putra RaharjoBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Horizontal Vertical MarketDokumen4 halamanHorizontal Vertical MarketVikasBelum ada peringkat
- Short Answers Class 9thDokumen14 halamanShort Answers Class 9thRizwan AliBelum ada peringkat
- 6470b0e5f337ed00180c05a4 - ## - Atomic Structure - DPP-01 (Of Lec-03) - Arjuna NEET 2024Dokumen3 halaman6470b0e5f337ed00180c05a4 - ## - Atomic Structure - DPP-01 (Of Lec-03) - Arjuna NEET 2024Lalit SinghBelum ada peringkat
- Effect of Dust On The Performance of Wind Turbines PDFDokumen12 halamanEffect of Dust On The Performance of Wind Turbines PDFJallal ArramachBelum ada peringkat
- Writing Simple Sentences to Describe ScenariosDokumen5 halamanWriting Simple Sentences to Describe Scenariosepol67% (3)
- 4D - Yulianti Viviana - Exercise 9Dokumen7 halaman4D - Yulianti Viviana - Exercise 9Uli JennerBelum ada peringkat
- Kanavos Pharmaceutical Distribution Chain 2007 PDFDokumen121 halamanKanavos Pharmaceutical Distribution Chain 2007 PDFJoao N Da SilvaBelum ada peringkat
- STS Syllabus 2020Dokumen27 halamanSTS Syllabus 2020AndreaDimaculangan100% (1)
- Simulated Robot Football Team Uses Neural Networks to LearnDokumen8 halamanSimulated Robot Football Team Uses Neural Networks to LearnKishore MuthukulathuBelum ada peringkat
- RoutineHub - R Download - iOS 13, 14, 15, 2Dokumen1 halamanRoutineHub - R Download - iOS 13, 14, 15, 2Gabriell AnjosBelum ada peringkat
- Sight Reduction Tables For Marine Navigation: B, R - D, D. SDokumen12 halamanSight Reduction Tables For Marine Navigation: B, R - D, D. SGeani MihaiBelum ada peringkat
- Arts9 q4 Mod1 Theatricalforms v5Dokumen30 halamanArts9 q4 Mod1 Theatricalforms v5Harold RicafortBelum ada peringkat
- Occupant Load CalculationsDokumen60 halamanOccupant Load CalculationsKAIVALYA TIWATNEBelum ada peringkat
- Axel LeijonhufvudDokumen7 halamanAxel LeijonhufvudDario CoceresBelum ada peringkat
- Tutorial Backpropagation Neural NetworkDokumen10 halamanTutorial Backpropagation Neural NetworkHeru PraBelum ada peringkat
- J-Garlic in CheeseDokumen12 halamanJ-Garlic in CheeseMary GinetaBelum ada peringkat
- OS9000 AOS 6.1.5 R01 Network Configuration GuideDokumen846 halamanOS9000 AOS 6.1.5 R01 Network Configuration GuideclaupasinaBelum ada peringkat
- Vonovia 9M2021 Presentation 20211118Dokumen76 halamanVonovia 9M2021 Presentation 20211118LorenzoBelum ada peringkat
- 04 LimeDokumen32 halaman04 LimeGoogle user100% (1)
- Current Developments in Testing Item Response Theory (IRT) : Prepared byDokumen32 halamanCurrent Developments in Testing Item Response Theory (IRT) : Prepared byMalar VengadesBelum ada peringkat
- 09 Chapter TeyyamDokumen48 halaman09 Chapter TeyyamABBelum ada peringkat
- TOS 22402 Winter 19th I SCHEME Paper Model Answer PaperDokumen25 halamanTOS 22402 Winter 19th I SCHEME Paper Model Answer Paperirshadmirza753Belum ada peringkat
- Amway Final ReportDokumen74 halamanAmway Final ReportRadhika Malhotra75% (4)
- Ubiquiti Af60-Xr DatasheetDokumen3 halamanUbiquiti Af60-Xr Datasheetayman rifaiBelum ada peringkat
- Barry Wylant: Design Thinking and The Experience of InnovationDokumen13 halamanBarry Wylant: Design Thinking and The Experience of InnovationVanesa JuarezBelum ada peringkat
- Surface water drainage infiltration testingDokumen8 halamanSurface water drainage infiltration testingRay CooperBelum ada peringkat
- History shapes Philippine societyDokumen4 halamanHistory shapes Philippine societyMarvin GwapoBelum ada peringkat
- Rock Type Identification Flow Chart: Sedimentary SedimentaryDokumen8 halamanRock Type Identification Flow Chart: Sedimentary Sedimentarymeletiou stamatiosBelum ada peringkat
- Judges - God's War Against HumanismDokumen347 halamanJudges - God's War Against HumanismgypsylanternBelum ada peringkat
- Loverpreet Chapterv 1Dokumen16 halamanLoverpreet Chapterv 1Sheikh SiddiquiBelum ada peringkat