Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- PESCI Recalls PDFDokumen9 halamanPESCI Recalls PDFDanishBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Organization of NICU ServicesDokumen45 halamanOrganization of NICU ServicesMonika Bagchi84% (64)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- McComb Letter On May 24, 2022, Port MeetingDokumen3 halamanMcComb Letter On May 24, 2022, Port MeetingcallertimesBelum ada peringkat
- 319th District Court Judge David Stitch Order of RecusalDokumen1 halaman319th District Court Judge David Stitch Order of RecusalcallertimesBelum ada peringkat
- Corpus Christi Tax Abatement Economic Analysis Report (With Appendix Update)Dokumen152 halamanCorpus Christi Tax Abatement Economic Analysis Report (With Appendix Update)callertimesBelum ada peringkat
- POCC CEO Letter On Desal EffortsDokumen2 halamanPOCC CEO Letter On Desal EffortscallertimesBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- PsycN NBME FOrm 4 Key Points for Tardive Dyskinesia, Multiple Sclerosis, Narcolepsy, TCAsDokumen2 halamanPsycN NBME FOrm 4 Key Points for Tardive Dyskinesia, Multiple Sclerosis, Narcolepsy, TCAsChristine CassidyBelum ada peringkat
- The San Angelo Standard-Times' Jacob Conner DocumentsDokumen6 halamanThe San Angelo Standard-Times' Jacob Conner DocumentscallertimesBelum ada peringkat
- DMD FY 2024 Service PlanDokumen12 halamanDMD FY 2024 Service PlancallertimesBelum ada peringkat
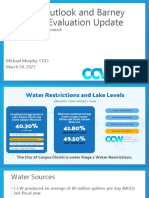
- Drought Outlook and Barney Davis Site Evaluation Update: For Corpus Christi City CouncilDokumen11 halamanDrought Outlook and Barney Davis Site Evaluation Update: For Corpus Christi City CouncilcallertimesBelum ada peringkat
- Bill Witt Aquatic Center PresentationDokumen8 halamanBill Witt Aquatic Center PresentationcallertimesBelum ada peringkat
- City Settlement With Ergon, ValeroDokumen32 halamanCity Settlement With Ergon, ValerocallertimesBelum ada peringkat
- OrderDokumen1 halamanOrdercallertimesBelum ada peringkat
- City Letter FHWADokumen42 halamanCity Letter FHWAcallertimesBelum ada peringkat
- Bohannon - Termination Notice 5.4.23Dokumen1 halamanBohannon - Termination Notice 5.4.23callertimesBelum ada peringkat
- Council Desal BriefDokumen11 halamanCouncil Desal BriefcallertimesBelum ada peringkat
- 46 Tex. Reg. 5447 (Aug. 27 2021)Dokumen1 halaman46 Tex. Reg. 5447 (Aug. 27 2021)callertimesBelum ada peringkat
- Padre Island National Seashore NewsletterDokumen6 halamanPadre Island National Seashore NewslettercallertimesBelum ada peringkat
- City of Corpus Christi's Bond Program GuideDokumen14 halamanCity of Corpus Christi's Bond Program GuidecallertimesBelum ada peringkat
- Letter Requesting Assignment From Missy MedaryDokumen1 halamanLetter Requesting Assignment From Missy MedarycallertimesBelum ada peringkat
- Order Denying Motion To Withdraw Execution of John Henry RamirezDokumen1 halamanOrder Denying Motion To Withdraw Execution of John Henry RamirezcallertimesBelum ada peringkat
- Ingleside On The Bay Coastal Watch Association On Permit WR13630Dokumen2 halamanIngleside On The Bay Coastal Watch Association On Permit WR13630callertimesBelum ada peringkat
- Letter of Clemency Denial To Attorney of John Henry RamirezDokumen1 halamanLetter of Clemency Denial To Attorney of John Henry RamirezcallertimesBelum ada peringkat
- Texas Commission On Jail Standards - Non Compliance 2022 For Nueces County JailDokumen2 halamanTexas Commission On Jail Standards - Non Compliance 2022 For Nueces County JailcallertimesBelum ada peringkat
- 2022 Caller Times Hurricane Preparedness GuideDokumen14 halaman2022 Caller Times Hurricane Preparedness GuidecallertimesBelum ada peringkat
- Nueces County Fire Marshal Resignation LetterDokumen1 halamanNueces County Fire Marshal Resignation LettercallertimesBelum ada peringkat
- Notice To Nueces County - ME's OfficeDokumen4 halamanNotice To Nueces County - ME's OfficecallertimesBelum ada peringkat
- City Letter Responding To POCC CEODokumen1 halamanCity Letter Responding To POCC CEOcallertimesBelum ada peringkat
- Jose Olivares TCOLE PCRDokumen14 halamanJose Olivares TCOLE PCRcallertimesBelum ada peringkat
- Proposed Game Room Regulations For Nueces CountyDokumen32 halamanProposed Game Room Regulations For Nueces CountycallertimesBelum ada peringkat
- Nueces County Game Room RegulationsDokumen24 halamanNueces County Game Room RegulationscallertimesBelum ada peringkat
- Letter To Port of Corpus Christi and City of Corpus ChristiDokumen2 halamanLetter To Port of Corpus Christi and City of Corpus ChristicallertimesBelum ada peringkat
- Planning Study, Nueces County PDO 2022Dokumen14 halamanPlanning Study, Nueces County PDO 2022callertimes100% (1)
- EN Quick Reference Guide Fabian HFOi-V4.0Dokumen30 halamanEN Quick Reference Guide Fabian HFOi-V4.0Tanzimul IslamBelum ada peringkat
- Impact of Estrogen Type On Cardiovascular Safety of Combined OralDokumen12 halamanImpact of Estrogen Type On Cardiovascular Safety of Combined OralMary SuescaBelum ada peringkat
- Varicella and Herpes ZosterDokumen20 halamanVaricella and Herpes ZosterzakiBelum ada peringkat
- PALS Helpful Hints 2015 Guidelines Posted Nov 2016Dokumen5 halamanPALS Helpful Hints 2015 Guidelines Posted Nov 2016Mj Teate100% (1)
- Psychiatric and Mental Health Nursing - Wikipedia PDFDokumen83 halamanPsychiatric and Mental Health Nursing - Wikipedia PDFJanani AmmuBelum ada peringkat
- Nursing Diagnosis and Plan of Care for Anemia with Chronic DiseaseDokumen6 halamanNursing Diagnosis and Plan of Care for Anemia with Chronic DiseaseChristine Joy FloresBelum ada peringkat
- Miliaria Pustulosa (Infetrop)Dokumen11 halamanMiliaria Pustulosa (Infetrop)Muhammad mukramBelum ada peringkat
- 2018 Conference AbstractsDokumen155 halaman2018 Conference AbstractsBanin AbadiBelum ada peringkat
- Drugs Acting On The Gastrointestinal System PDFDokumen18 halamanDrugs Acting On The Gastrointestinal System PDFMarc De JesusBelum ada peringkat
- Designed To Enhance From The Inside Out: Apd TherapyDokumen7 halamanDesigned To Enhance From The Inside Out: Apd TherapyNumael Alfonso Serrato AlvaradoBelum ada peringkat
- Guía OxigenoterapiaDokumen39 halamanGuía OxigenoterapiaSMIBA MedicinaBelum ada peringkat
- Implementasi PMKP di Rumah SakitDokumen29 halamanImplementasi PMKP di Rumah SakitikaoktaviasaktiBelum ada peringkat
- Nursing Documentation for Wina Purnamasari's Immunization and Vital Signs CheckDokumen6 halamanNursing Documentation for Wina Purnamasari's Immunization and Vital Signs Checkilah keciBelum ada peringkat
- Understanding Plasma Cell Dyscrasias: MGUS, Myeloma, Waldenstrom's and AmyloidosisDokumen41 halamanUnderstanding Plasma Cell Dyscrasias: MGUS, Myeloma, Waldenstrom's and AmyloidosisDr MonikaBelum ada peringkat
- Diabetes TrackerDokumen1 halamanDiabetes Trackerwildlifewarrior_zrsBelum ada peringkat
- Malignant Hyperthermia: Pre-Hospital Emergency Care Recommendations Recommendations For Hospital Emergency DepartmentsDokumen6 halamanMalignant Hyperthermia: Pre-Hospital Emergency Care Recommendations Recommendations For Hospital Emergency DepartmentsHelend Ndra TaribukaBelum ada peringkat
- Approved Private Hospitals List for CG Govt EmployeesDokumen12 halamanApproved Private Hospitals List for CG Govt Employeesm_asitBelum ada peringkat
- Cannabis-An IntroductionDokumen5 halamanCannabis-An IntroductionSaleha TariqBelum ada peringkat
- How To Protect Yourself and OthersDokumen2 halamanHow To Protect Yourself and OtherslistmyclinicBelum ada peringkat
- Sush Unity Haemotology-1700Dokumen51 halamanSush Unity Haemotology-1700Dr-Jahanzaib GondalBelum ada peringkat
- Standards of Medical Care in Diabetes-2022Dokumen10 halamanStandards of Medical Care in Diabetes-2022Adina SimionBelum ada peringkat
- Insights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityDokumen4 halamanInsights Into Veterinary Endocrinology - Diagnostic Approach To PU - PD - Urine Specific GravityHusnat hussainBelum ada peringkat
- 4-5TH JANUARY 2023: Organized byDokumen3 halaman4-5TH JANUARY 2023: Organized byvivien kate perixBelum ada peringkat
- BiopharmaceuticsDokumen52 halamanBiopharmaceuticsDharma ShantiniBelum ada peringkat
- German Gov't Bombshell - Alarming Number of Vaccinated Are Developing AIDS' - News PunchDokumen8 halamanGerman Gov't Bombshell - Alarming Number of Vaccinated Are Developing AIDS' - News PunchKarla VegaBelum ada peringkat
- ImgDokumen1 halamanImgLIDIYA MOL P V100% (1)
- Living With CancerDokumen400 halamanLiving With CancerAnonymous FGqnrDuMBelum ada peringkat