Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
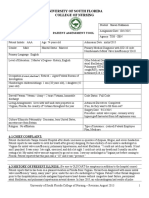
- Pediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467LDokumen4 halamanPediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467Lapi-324566318Belum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Picu WorksheetDokumen7 halamanPicu Worksheetapi-324566318Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Pat 2 - Semester 2Dokumen27 halamanPat 2 - Semester 2api-324566318Belum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Pediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467LDokumen4 halamanPediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467Lapi-324566318Belum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Portfolio-Goals PaperDokumen2 halamanPortfolio-Goals Paperapi-324566318Belum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Discssion EbpDokumen4 halamanDiscssion Ebpapi-324566318Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Nicu Worksheet CompletedDokumen3 halamanNicu Worksheet Completedapi-324566318Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Portfolio-Clinical ExemplarDokumen4 halamanPortfolio-Clinical Exemplarapi-324566318Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Pat 1 Semester 2 TGH SBN Hekkanen ShawnDokumen23 halamanPat 1 Semester 2 TGH SBN Hekkanen Shawnapi-324566318Belum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Final Draft Discussion Board 3-EthicsDokumen3 halamanFinal Draft Discussion Board 3-Ethicsapi-324566318Belum ada peringkat
- Synthesis Summative-Hekkanen ShawnDokumen11 halamanSynthesis Summative-Hekkanen Shawnapi-324566318Belum ada peringkat
- Cultural Paper Cut Hekkanen Shawn 2Dokumen5 halamanCultural Paper Cut Hekkanen Shawn 2api-324566318Belum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Policy Paper2 Hekkanen ShawnDokumen12 halamanPolicy Paper2 Hekkanen Shawnapi-324566318Belum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Patient Safety Quality Care Movement-Leadership Abridged For DataDokumen8 halamanPatient Safety Quality Care Movement-Leadership Abridged For Dataapi-324566318Belum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Portfolio-Evaluation AnecdotalDokumen10 halamanPortfolio-Evaluation Anecdotalapi-324566318Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Portfolio-Evaluation NPWDokumen2 halamanPortfolio-Evaluation NPWapi-324566318Belum ada peringkat
- Portfolio-Evaluation Final 1Dokumen3 halamanPortfolio-Evaluation Final 1api-324566318Belum ada peringkat
- Portfolio-Certifications HorizontalDokumen4 halamanPortfolio-Certifications Horizontalapi-324566318Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- India Immunization Chart 2010Dokumen1 halamanIndia Immunization Chart 2010Sarath Nageshwaran SujathaBelum ada peringkat
- Arthrogryposis Multiplex Congenita (AMC) in Siblings - Case Report. First DCMS Annual Research Day, April 7, 2018Dokumen8 halamanArthrogryposis Multiplex Congenita (AMC) in Siblings - Case Report. First DCMS Annual Research Day, April 7, 2018Razi MohdBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- 2016 - Byk FotoDokumen7 halaman2016 - Byk FotoSyifa IKBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Acute Compartment SyndromeDokumen44 halamanAcute Compartment Syndromeasi basseyBelum ada peringkat
- Dr. Hossam Eldin Sayed Ali: Lecturer of Medical Biophysics The Research Institute of OphthalmologyDokumen32 halamanDr. Hossam Eldin Sayed Ali: Lecturer of Medical Biophysics The Research Institute of OphthalmologyRiya MathurBelum ada peringkat
- NstiDokumen12 halamanNstiKania IradatyaBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- 113 - JCI Mock Survey QuestionDokumen4 halaman113 - JCI Mock Survey QuestionMohamad Attia100% (1)
- Atrium MedicalDokumen12 halamanAtrium MedicalBo TaoBelum ada peringkat
- Kelly: The Patient's PageDokumen4 halamanKelly: The Patient's PageMegi PavletićBelum ada peringkat
- Dementia Conversion DisordersDokumen28 halamanDementia Conversion DisordersAYO NELSON100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Cryptogenic StrokeDokumen17 halamanCryptogenic StrokeIRENA GENIBelum ada peringkat
- Pathophysiology - PyelonephritisDokumen2 halamanPathophysiology - PyelonephritisFrancis Kevin Sagudo92% (13)
- Pediatric Anesthesiology PDFDokumen309 halamanPediatric Anesthesiology PDFAviv Pasa100% (1)
- Anorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesDokumen31 halamanAnorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesCarito Hernandez RodriguezBelum ada peringkat
- Vaccination Records - AdultsDokumen2 halamanVaccination Records - AdultsverumluxBelum ada peringkat
- The Sage Encyclopedia of Abnormal and Clinical Psychology - I36172Dokumen5 halamanThe Sage Encyclopedia of Abnormal and Clinical Psychology - I36172Rol AnimeBelum ada peringkat
- Jurnal Vitamin CDokumen15 halamanJurnal Vitamin CbethjohBelum ada peringkat
- AstrocytomaDokumen3 halamanAstrocytomaShamae PatalinjugBelum ada peringkat
- "HIV Depletes T-Helper17, We Simply Stimulate It": by Prof. DR - Pichaet Wiriyachitra PH.D., F.R.A.C.IDokumen37 halaman"HIV Depletes T-Helper17, We Simply Stimulate It": by Prof. DR - Pichaet Wiriyachitra PH.D., F.R.A.C.IfroggyzzBelum ada peringkat
- Daftar Pustaka Presentasi BokongDokumen2 halamanDaftar Pustaka Presentasi BokongNando UspessyBelum ada peringkat
- Mandala Coloring For Children With Symptoms of Attention Deficit Hyperactivity Disorder - A Case SeriesDokumen7 halamanMandala Coloring For Children With Symptoms of Attention Deficit Hyperactivity Disorder - A Case Seriesindex PubBelum ada peringkat
- Kumar Fong's Prescription WorksheetDokumen2 halamanKumar Fong's Prescription WorksheetKumar fongBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Ketamin FarmakologiDokumen19 halamanKetamin FarmakologiBang mantoBelum ada peringkat
- Alzheimer's Disease (AD), Also Referred To Simply As Alzheimer's, Is ADokumen2 halamanAlzheimer's Disease (AD), Also Referred To Simply As Alzheimer's, Is ASCrIbdBelum ada peringkat
- Isicem 2021Dokumen90 halamanIsicem 2021labbeneBelum ada peringkat
- Bitter PrinciplesDokumen6 halamanBitter PrinciplesPankaj BudhlakotiBelum ada peringkat
- Stepwise Ventilator Waveform Assessment To Diagnose Pulmonary PathophysiologyDokumen8 halamanStepwise Ventilator Waveform Assessment To Diagnose Pulmonary PathophysiologyPablo Simón Narbona MenaBelum ada peringkat
- Nclex Past QuestionsDokumen452 halamanNclex Past Questionsjyka100% (21)
- (Board Review Series) Linda S. Costanzo - BRS Physiology, 5th Edition (Board Review Series) - Lippincott Williams & Wilkins (2010)Dokumen7 halaman(Board Review Series) Linda S. Costanzo - BRS Physiology, 5th Edition (Board Review Series) - Lippincott Williams & Wilkins (2010)Salifyanji SimpambaBelum ada peringkat
- Graves DiseaseDokumen7 halamanGraves DiseaseNader SmadiBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (402)