Anda mungkin juga menyukai
- Myelography PDFDokumen13 halamanMyelography PDFAhmad HaririBelum ada peringkat
- Allied Health Professionals: Mutual Recognition ApplicationDokumen3 halamanAllied Health Professionals: Mutual Recognition ApplicationAhmad HaririBelum ada peringkat
- JCI Newsletter May 8 IPSGDokumen6 halamanJCI Newsletter May 8 IPSGAhmad HaririBelum ada peringkat
- Pengenalan CT ScanDokumen2 halamanPengenalan CT ScanAhmad HaririBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Permutation PolynomialsDokumen64 halamanPermutation Polynomialsmestrado unbBelum ada peringkat
- Executive Incentives and The Horizon Problem An - 1991 - Journal of AccountingDokumen39 halamanExecutive Incentives and The Horizon Problem An - 1991 - Journal of AccountingYuhan JiBelum ada peringkat
- Programming For Problem SolvingDokumen5 halamanProgramming For Problem SolvingAPOLLO Sem 4 I.T.Belum ada peringkat
- Psychometric Development and Validation of GaslightingDokumen15 halamanPsychometric Development and Validation of GaslightingYang ZhangBelum ada peringkat
- Physical Quantities and Unit: 9th GradeDokumen28 halamanPhysical Quantities and Unit: 9th GradeAlexanderBelum ada peringkat
- FST 3000Dokumen4 halamanFST 3000ariksyaiful82Belum ada peringkat
- Homeassignment 4 (1) (1) - 2Dokumen3 halamanHomeassignment 4 (1) (1) - 2hellokaun1072Belum ada peringkat
- Cat Hammers C842898Dokumen8 halamanCat Hammers C842898maggioraBelum ada peringkat
- 4$20 Triangles$20 ProofsDokumen23 halaman4$20 Triangles$20 ProofsBaskaran SeetharamanBelum ada peringkat
- Development and Experimental Evaluation of Machine Learning Techniques For An Intelligent Hairy Scalp Detection SystemDokumen29 halamanDevelopment and Experimental Evaluation of Machine Learning Techniques For An Intelligent Hairy Scalp Detection SystemBilly GeneBelum ada peringkat
- Zbrush 4 ShortcutsDokumen3 halamanZbrush 4 ShortcutsJBelum ada peringkat
- AtomDokumen15 halamanAtomdewi murtasimaBelum ada peringkat
- ASUS U47A Repair GuideDokumen5 halamanASUS U47A Repair GuideCarlos ZarateBelum ada peringkat
- 144S... - PCB Series: Signal Conditioned Precision Pressure TransducersDokumen4 halaman144S... - PCB Series: Signal Conditioned Precision Pressure TransducersAnish KumarBelum ada peringkat
- Nav 2000Dokumen4 halamanNav 2000Balaji TriplantBelum ada peringkat
- BSS - Report - Effect of Heat in A Building DemonstratorDokumen15 halamanBSS - Report - Effect of Heat in A Building DemonstratorAh Mok100% (1)
- RWC 123 Manoj Prabhakar KaiwartDokumen13 halamanRWC 123 Manoj Prabhakar KaiwartManoj Prabhakar KaiwartBelum ada peringkat
- Rekonfigurasi Jaringan Distribusi Radial Untuk Mengurangi Rugi Daya Pada Penyulang Jatirejo Rayon Mojoagung Menggunakan Metode BinaryDokumen4 halamanRekonfigurasi Jaringan Distribusi Radial Untuk Mengurangi Rugi Daya Pada Penyulang Jatirejo Rayon Mojoagung Menggunakan Metode BinaryNurindra CahyantaBelum ada peringkat
- Installation, Operation, and Maintenance ManualDokumen54 halamanInstallation, Operation, and Maintenance ManualIsmael Berlanga ResBelum ada peringkat
- Helmholtz Resonance - Wikipedia, The Free EncyclopediaDokumen4 halamanHelmholtz Resonance - Wikipedia, The Free Encyclopediahamidah1963Belum ada peringkat
- SC431 Lecture No. 4 Economic Comparisons (Continued)Dokumen51 halamanSC431 Lecture No. 4 Economic Comparisons (Continued)Joseph BaruhiyeBelum ada peringkat
- Binary PDFDokumen13 halamanBinary PDFbyprasadBelum ada peringkat
- Sti260N6F6 Stp260N6F6: N-Channel 60 V, 0.0024 Ω, 120 A Stripfet™ Vi Deepgate™ Power Mosfet In To-220 And I²Pak PackagesDokumen14 halamanSti260N6F6 Stp260N6F6: N-Channel 60 V, 0.0024 Ω, 120 A Stripfet™ Vi Deepgate™ Power Mosfet In To-220 And I²Pak PackagesRyn YahuFBelum ada peringkat
- TOFD Dead Zone CalculatorDokumen4 halamanTOFD Dead Zone CalculatorWill SmithBelum ada peringkat
- Origin and Structure of The EarthDokumen8 halamanOrigin and Structure of The EarthRobin Suarez ViladoBelum ada peringkat
- UNIT 14 - On-Screen DigitizingDokumen6 halamanUNIT 14 - On-Screen DigitizingResti KharismaBelum ada peringkat
- Petrom OMV Norm DEF 2001 Rom Eng Rev.2 2009-06-01Dokumen61 halamanPetrom OMV Norm DEF 2001 Rom Eng Rev.2 2009-06-01luciandu100% (1)
- Coding Assignment 18-WPS OfficeDokumen9 halamanCoding Assignment 18-WPS Officetamj tamjBelum ada peringkat
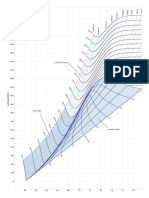
- Mollier Enthalpy Entropy Chart For Steam - US UnitsDokumen1 halamanMollier Enthalpy Entropy Chart For Steam - US Unitslin tongBelum ada peringkat
- FlopX NT5.1 Patch V1aDokumen5 halamanFlopX NT5.1 Patch V1aAmilcar AndradeBelum ada peringkat