Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Reverse Circulation Cementing: The Complete PictureDokumen104 halamanReverse Circulation Cementing: The Complete PictureJoan Corso100% (1)
- 3700 RES 5.5.1 Install GuideDokumen38 halaman3700 RES 5.5.1 Install Guidejlappi100% (1)
- Eview: Alternative Polyadenylation: A Twist On mRNA 3 End FormationDokumen9 halamanEview: Alternative Polyadenylation: A Twist On mRNA 3 End FormationdupuytrenBelum ada peringkat
- Adenovirus Production ProtocolDokumen13 halamanAdenovirus Production ProtocoldupuytrenBelum ada peringkat
- Heat Inactivation ProtocolDokumen1 halamanHeat Inactivation ProtocoldupuytrenBelum ada peringkat
- Microtubules in SynapseDokumen6 halamanMicrotubules in SynapsedupuytrenBelum ada peringkat
- Fluorescence and Fluorescence ApplicationsDokumen13 halamanFluorescence and Fluorescence ApplicationsPaulraj Mosae SelvakumarBelum ada peringkat
- Lentivirus Production ProtocolDokumen11 halamanLentivirus Production ProtocoldupuytrenBelum ada peringkat
- Genome-Wide Alternative Polyadenylation in Animals: Insights From High-Throughput TechnologiesDokumen10 halamanGenome-Wide Alternative Polyadenylation in Animals: Insights From High-Throughput TechnologiesdupuytrenBelum ada peringkat
- Non-Genetic Inheritance Via The Male Germline in Mammals: ReviewDokumen7 halamanNon-Genetic Inheritance Via The Male Germline in Mammals: ReviewdupuytrenBelum ada peringkat
- Simplicon Rna Reprogramming - PrinterviewDokumen5 halamanSimplicon Rna Reprogramming - PrinterviewdupuytrenBelum ada peringkat
- Adhesion Signalling Complexes: PrimerDokumen5 halamanAdhesion Signalling Complexes: PrimerdupuytrenBelum ada peringkat
- An Integrative Framework For Understanding The Mechanisms and Multigenerational Consequences of Transgenerational PlasticityDokumen22 halamanAn Integrative Framework For Understanding The Mechanisms and Multigenerational Consequences of Transgenerational PlasticitydupuytrenBelum ada peringkat
- Direct Comparison of Dna Versus Mrna On The Efficiency of Induced Pluripotent Stem Cells Generation From Human Primary FibroblastsDokumen7 halamanDirect Comparison of Dna Versus Mrna On The Efficiency of Induced Pluripotent Stem Cells Generation From Human Primary FibroblastsdupuytrenBelum ada peringkat
- Dynamics of Epigenetic Phenomena: Intergenerational and Intragenerational Phenotype Washout'Dokumen8 halamanDynamics of Epigenetic Phenomena: Intergenerational and Intragenerational Phenotype Washout'dupuytrenBelum ada peringkat
- Uncovering Cell Biology in The Third DimensionDokumen5 halamanUncovering Cell Biology in The Third DimensiondupuytrenBelum ada peringkat
- Echinocandins: The Newest Class of Antifungals: Infectious DiseasesDokumen11 halamanEchinocandins: The Newest Class of Antifungals: Infectious DiseasesdupuytrenBelum ada peringkat
- Focal Adhesions in Osteoneogenesis: Special Issue Paper 1441Dokumen13 halamanFocal Adhesions in Osteoneogenesis: Special Issue Paper 1441dupuytrenBelum ada peringkat
- 5550 FullDokumen8 halaman5550 FulldupuytrenBelum ada peringkat
- Studying Hallmarks of Cancer - AbcamDokumen11 halamanStudying Hallmarks of Cancer - AbcamdupuytrenBelum ada peringkat
- 8927 FullDokumen5 halaman8927 FulldupuytrenBelum ada peringkat
- Stemcells 2006-0409Dokumen9 halamanStemcells 2006-0409dupuytrenBelum ada peringkat
- Perspectives: Applying CRISPR-Cas9 Tools To Identify and Characterize Transcriptional EnhancersDokumen8 halamanPerspectives: Applying CRISPR-Cas9 Tools To Identify and Characterize Transcriptional EnhancersdupuytrenBelum ada peringkat
- NT 82908Dokumen3 halamanNT 82908Jaya KumarBelum ada peringkat
- New Drugs 2017Dokumen2 halamanNew Drugs 2017dupuytrenBelum ada peringkat
- Treatment of Antineutrophil Cytoplasmic Antibodyassociated VasculitisDokumen8 halamanTreatment of Antineutrophil Cytoplasmic Antibodyassociated VasculitisdupuytrenBelum ada peringkat
- Cellular Viability - Calcein / Propidium Iodide: We've Performed This Assay On The Following Cell TypesDokumen1 halamanCellular Viability - Calcein / Propidium Iodide: We've Performed This Assay On The Following Cell TypesdupuytrenBelum ada peringkat
- Cold Spring Harb Protoc-2011-Matheu-pdb - Prot5565Dokumen6 halamanCold Spring Harb Protoc-2011-Matheu-pdb - Prot5565dupuytrenBelum ada peringkat
- Commercialization of Organoids: ForumDokumen4 halamanCommercialization of Organoids: ForumdupuytrenBelum ada peringkat
- Pioneer Transcription Factors in Cell Fate ControlDokumen5 halamanPioneer Transcription Factors in Cell Fate ControldupuytrenBelum ada peringkat
- Preliminary MatterDokumen26 halamanPreliminary MatterdupuytrenBelum ada peringkat
- Neuroview: How To Be A Graduate AdviseeDokumen3 halamanNeuroview: How To Be A Graduate AdviseedupuytrenBelum ada peringkat
- Exercise 1 - Revision StringDokumen2 halamanExercise 1 - Revision StringKu H6Belum ada peringkat
- P 130881757895329843Dokumen44 halamanP 130881757895329843Vijay MohanBelum ada peringkat
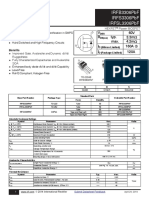
- Irfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADokumen12 halamanIrfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADirson Volmir WilligBelum ada peringkat
- TitleDokumen142 halamanTitleAmar PašićBelum ada peringkat
- 1.summative-Test Math7Dokumen1 halaman1.summative-Test Math7Jaylor GaridoBelum ada peringkat
- Residual Alkalinity Nomograph by John Palmer PDFDokumen1 halamanResidual Alkalinity Nomograph by John Palmer PDFcarlos pablo pableteBelum ada peringkat
- Food Preparation, Terms and DefinitiosDokumen2 halamanFood Preparation, Terms and DefinitiosLacsi, Erica Joy V.Belum ada peringkat
- Flexenclosure Esite Brochure PDFDokumen5 halamanFlexenclosure Esite Brochure PDFajdCruiseBelum ada peringkat
- Watchgas AirWatch MK1.0 Vs MK1.2Dokumen9 halamanWatchgas AirWatch MK1.0 Vs MK1.2elliotmoralesBelum ada peringkat
- Ergonomic DesignDokumen132 halamanErgonomic DesignErin WalkerBelum ada peringkat
- CFMDokumen16 halamanCFMShoaibIqbalBelum ada peringkat
- Solution To QuestionsDokumen76 halamanSolution To QuestionsVipul AggarwalBelum ada peringkat
- Aluminum: DR 900 Analytical ProcedureDokumen4 halamanAluminum: DR 900 Analytical Procedurewulalan wulanBelum ada peringkat
- The Big TEGO. Products Services Data Sheets-75-150-16!76!31-61Dokumen31 halamanThe Big TEGO. Products Services Data Sheets-75-150-16!76!31-61DWI RAHMASARI FATMAWATIBelum ada peringkat
- Chapter 6 - Process Capability AnalysisDokumen21 halamanChapter 6 - Process Capability AnalysisKaya Eralp AsanBelum ada peringkat
- RomerDokumen20 halamanRomerAkistaaBelum ada peringkat
- Budget of Work Sci5Dokumen1 halamanBudget of Work Sci5Jhoy Angeles PinlacBelum ada peringkat
- Power Electronics Circuits Devices and Applications by Muhammad H RashidDokumen602 halamanPower Electronics Circuits Devices and Applications by Muhammad H Rashidkartik balojiBelum ada peringkat
- Wacker Neuson Light Towers LTN 6l Parts Manual 348628422Dokumen23 halamanWacker Neuson Light Towers LTN 6l Parts Manual 348628422kellyholland180884pnc100% (61)
- Teaching Tactics and Teaching Strategy: Arthur W. Foshay'Dokumen4 halamanTeaching Tactics and Teaching Strategy: Arthur W. Foshay'Ahmed DaibecheBelum ada peringkat
- Magnetism NotesDokumen14 halamanMagnetism Notesapi-277818647Belum ada peringkat
- Tutoriales Mastercam V8 6-11Dokumen128 halamanTutoriales Mastercam V8 6-11Eduardo Felix Ramirez PalaciosBelum ada peringkat
- Lecture 8cDokumen29 halamanLecture 8cs_paraisoBelum ada peringkat
- Fongs ProgrammerDokumen5 halamanFongs ProgrammerPankaj PolaraBelum ada peringkat
- Chapter 16 - Oral Radiography (Essentials of Dental Assisting)Dokumen96 halamanChapter 16 - Oral Radiography (Essentials of Dental Assisting)mussanteBelum ada peringkat
- Chap006 - Process Selection & Facility Layout-1Dokumen48 halamanChap006 - Process Selection & Facility Layout-1Ohud AlanaziBelum ada peringkat
- Solenoid ValveDokumen76 halamanSolenoid ValveazlanBelum ada peringkat
- Lab1: Access Control: Posix AclDokumen7 halamanLab1: Access Control: Posix AclAla JebnounBelum ada peringkat