Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Career Opportunities in NursingDokumen16 halamanCareer Opportunities in NursingRani100% (5)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- CCN (Critical Care Nursing)Dokumen4 halamanCCN (Critical Care Nursing)Laurence ZernaBelum ada peringkat
- Log Book IdccmDokumen38 halamanLog Book IdccmAnish H Dave50% (2)
- International Case StudyDokumen36 halamanInternational Case Studymamona zaheerBelum ada peringkat
- New Assessment Tool Level 2 Hospital PDFDokumen18 halamanNew Assessment Tool Level 2 Hospital PDFMaridel JuenBelum ada peringkat
- Ijmr Tetanus in 2 Yo PDFDokumen4 halamanIjmr Tetanus in 2 Yo PDFvidyahamzahBelum ada peringkat
- CHF (Diagnosis, Patophysiology, Therapy, and Implication For Respiratory Care)Dokumen10 halamanCHF (Diagnosis, Patophysiology, Therapy, and Implication For Respiratory Care)blobfish_danboBelum ada peringkat
- 4398 8451 1 SM PDFDokumen9 halaman4398 8451 1 SM PDFKavita FairuzBelum ada peringkat
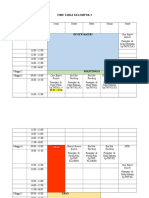
- Time Table Kelompok 2Dokumen3 halamanTime Table Kelompok 2vidyahamzahBelum ada peringkat
- CataractDokumen26 halamanCataractHasnan HabibBelum ada peringkat
- LGBT or GLBT Is AnDokumen2 halamanLGBT or GLBT Is AnvidyahamzahBelum ada peringkat
- 2049 9752 5 2Dokumen7 halaman2049 9752 5 2BillGhoes'toBelum ada peringkat
- Unusual Airway Situation, Esophageal Stethoscope Knotted AroundDokumen2 halamanUnusual Airway Situation, Esophageal Stethoscope Knotted AroundvidyahamzahBelum ada peringkat
- 2049 9752 2 25Dokumen5 halaman2049 9752 2 25dewi_s_3Belum ada peringkat
- 2015 AHA Guidelines Highlights EnglishDokumen36 halaman2015 AHA Guidelines Highlights EnglishshiloinBelum ada peringkat
- SOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticDokumen5 halamanSOFA (Sequential Organ Failure Assessment) and PELOD (Pediatric LogisticvidyahamzahBelum ada peringkat
- Fss-Icu An Outcome Worth MeasuringDokumen15 halamanFss-Icu An Outcome Worth Measuringapi-703723590Belum ada peringkat
- Pediatric Medical DevicesDokumen25 halamanPediatric Medical DevicesDuck Mann-ConsulBelum ada peringkat
- Fluid Response Evaluation in Sepsis Hypotension and Shock A Randomized Clinical TrialDokumen15 halamanFluid Response Evaluation in Sepsis Hypotension and Shock A Randomized Clinical TrialntnquynhproBelum ada peringkat
- Tell The World Project WC EditDokumen3 halamanTell The World Project WC Editapi-473913057Belum ada peringkat
- J Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The AdultDokumen30 halamanJ Parenter Enteral Nutr - 2021 - Compher - Guidelines For The Provision of Nutrition Support Therapy in The Adultsulemi castañonBelum ada peringkat
- American Journal of Respiratory and Critical Care MedicineDokumen12 halamanAmerican Journal of Respiratory and Critical Care MedicineChanya ChomchoeyBelum ada peringkat
- Weaning ProtocolDokumen6 halamanWeaning ProtocolerwanBelum ada peringkat
- Accelerating System Thinking in Health SystemsDokumen23 halamanAccelerating System Thinking in Health SystemsFadhila Nurfajrina100% (1)
- ALVO Mobile HospitalDokumen8 halamanALVO Mobile HospitalGUSTAVO el canal de youtubeBelum ada peringkat
- Australasian Emergency Care: Happy I. Kusumawati, Judy Magarey, Philippa RasmussenDokumen6 halamanAustralasian Emergency Care: Happy I. Kusumawati, Judy Magarey, Philippa Rasmussenrida rahmayantiBelum ada peringkat
- ANP CASE PRESENTATION OF ICU 101 ShilpaDokumen23 halamanANP CASE PRESENTATION OF ICU 101 ShilpaShilpa JoshiBelum ada peringkat
- Emily Morgan - ResumeDokumen2 halamanEmily Morgan - Resumeapi-283578734Belum ada peringkat
- Hospital Assessment ToolDokumen68 halamanHospital Assessment ToolXylia TocaoBelum ada peringkat
- Materi B. InggrisDokumen9 halamanMateri B. Inggrisdita novia maharaniBelum ada peringkat
- The Guitar in MTDokumen20 halamanThe Guitar in MTDorcas WongBelum ada peringkat
- The Organization of Internal Management ConsultancyDokumen8 halamanThe Organization of Internal Management ConsultancyBenjamin C. OkoroaforBelum ada peringkat
- Alex Hardin Resume 2015Dokumen3 halamanAlex Hardin Resume 2015api-306883462Belum ada peringkat
- Bicar IcuDokumen10 halamanBicar Icuhemodiálise NIRBelum ada peringkat
- Adnan - Abdi 2Dokumen65 halamanAdnan - Abdi 2Shükrî ÆbBelum ada peringkat
- Indianbank Policy WordingsDokumen32 halamanIndianbank Policy WordingsRaja KatareBelum ada peringkat
- Flannery 2016Dokumen10 halamanFlannery 2016mohamad safiiBelum ada peringkat
- Uoi Affidavit 9052021 Final With Annexures 1 91 393168Dokumen91 halamanUoi Affidavit 9052021 Final With Annexures 1 91 393168RUDRAA HIRANWARBelum ada peringkat
- Tutorials / Workshops: 9th Annual Critical Care SymposiumDokumen2 halamanTutorials / Workshops: 9th Annual Critical Care SymposiumredmondptBelum ada peringkat
- Inferior Vena Cava Diameter and Collapsibility IndexDokumen9 halamanInferior Vena Cava Diameter and Collapsibility IndexmalisalukmanBelum ada peringkat
- Achmad R. Muttaqien Cost Effectiveness of Intensive Care in A Low Resource Setting A Prospective Cohort of Medical Critically Ill PatientsDokumen17 halamanAchmad R. Muttaqien Cost Effectiveness of Intensive Care in A Low Resource Setting A Prospective Cohort of Medical Critically Ill PatientsAchmad R. MuttaqienBelum ada peringkat