Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Clinical Cases For MRCPCH PART 2 Applied Knowledge in PracticeDokumen218 halamanClinical Cases For MRCPCH PART 2 Applied Knowledge in Practiceaeyousef88% (16)
- DRUG STUDY PsycheDokumen1 halamanDRUG STUDY Psychejulesubayubay5428100% (1)
- Chinchu JosephDokumen169 halamanChinchu JosephMerinBelum ada peringkat
- 861 Drug Prescribing For Dentistry 2 Web 2 Email PDFDokumen94 halaman861 Drug Prescribing For Dentistry 2 Web 2 Email PDFRaphaela TravassosBelum ada peringkat
- MCQ on Types of GlomerulonephritisDokumen3 halamanMCQ on Types of GlomerulonephritisIM CT50% (2)
- Pediatric Urinary Tract Infections PDFDokumen30 halamanPediatric Urinary Tract Infections PDFMirunaBurceaBelum ada peringkat
- Infecºiile Tractului Urinar La Copil: Clinica de Pediatrie, Spitalul Clinic de Copii Dr. V. Gomoiu", Bucure¿tiDokumen15 halamanInfecºiile Tractului Urinar La Copil: Clinica de Pediatrie, Spitalul Clinic de Copii Dr. V. Gomoiu", Bucure¿tiMirunaBurceaBelum ada peringkat
- Effects of Scaling and Root Planing On Clinical Response and Serum Levels of Adipocytokines in Patients With Obesity and Chronic PeriodontitisDokumen9 halamanEffects of Scaling and Root Planing On Clinical Response and Serum Levels of Adipocytokines in Patients With Obesity and Chronic PeriodontitisMirunaBurceaBelum ada peringkat
- 2.a Judicious Treatment Approach For The Management of Localized AggressiveDokumen4 halaman2.a Judicious Treatment Approach For The Management of Localized AggressiveMirunaBurceaBelum ada peringkat
- 1.periodontal Treatment Improves Prostate Symptoms and Lowers SerumDokumen4 halaman1.periodontal Treatment Improves Prostate Symptoms and Lowers SerumMirunaBurceaBelum ada peringkat
- Jomi 7657Dokumen27 halamanJomi 7657casto.carpetasmiaBelum ada peringkat
- Obstetrics and GynacologyDokumen14 halamanObstetrics and GynacologykalkidanBelum ada peringkat
- Comparison Between DOAC To Enoxaparin For Risk of Intracranial BleedingDokumen2 halamanComparison Between DOAC To Enoxaparin For Risk of Intracranial BleedingFathima Sheik KatherBelum ada peringkat
- 5a.ESOPHAGEAL DISORDERSDokumen16 halaman5a.ESOPHAGEAL DISORDERSHayat AL AKOUMBelum ada peringkat
- Not Eligible As No Experience of Teaching and ResearchDokumen5 halamanNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaBelum ada peringkat
- Hip Dislocation ResearchDokumen8 halamanHip Dislocation Researchapi-268839011Belum ada peringkat
- Delusional Jealusy - FullDokumen17 halamanDelusional Jealusy - FullnicolasBelum ada peringkat
- Morpho - Pathology Final Summary: Chapter 1: Cellular Reactions To AggressionDokumen21 halamanMorpho - Pathology Final Summary: Chapter 1: Cellular Reactions To Aggressiondjxela89Belum ada peringkat
- HomeostasisDokumen12 halamanHomeostasisTimothy StanleyBelum ada peringkat
- RNA Non Enveloped VirusesDokumen35 halamanRNA Non Enveloped VirusesRPh Krishna Chandra JagritBelum ada peringkat
- Autism and Dietary Therapy: Case Report and Review of The LiteratureDokumen6 halamanAutism and Dietary Therapy: Case Report and Review of The LiteratureAntiopi PanteliBelum ada peringkat
- Introduction To Nursing PharmacologyDokumen5 halamanIntroduction To Nursing PharmacologyJon Adam Bermudez SamatraBelum ada peringkat
- Journal BalakrishnaDokumen3 halamanJournal BalakrishnafandheanayaBelum ada peringkat
- Oral Health During Pregnancy - An Analysis of Information CoDokumen8 halamanOral Health During Pregnancy - An Analysis of Information CoElena IancuBelum ada peringkat
- 19 Spinal CordDokumen8 halaman19 Spinal Cordkarar AhmedBelum ada peringkat
- A Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostDokumen6 halamanA Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostIJRASETPublicationsBelum ada peringkat
- A Case Report On Sickle Cell Disease With Hemolyti PDFDokumen4 halamanA Case Report On Sickle Cell Disease With Hemolyti PDFAlhaji SwarrayBelum ada peringkat
- Electrocardiography Wave Analysis: Using MATLABDokumen19 halamanElectrocardiography Wave Analysis: Using MATLABSMBelum ada peringkat
- Significance of Facebow Transfer: January 2020Dokumen6 halamanSignificance of Facebow Transfer: January 2020Mahmoud Ibrahem maanBelum ada peringkat
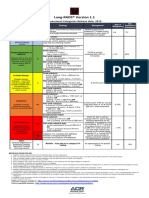
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokumen1 halamanLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotBelum ada peringkat
- QuestionsDokumen6 halamanQuestionsLorvic Andrew Juanson UmaliBelum ada peringkat
- MSUDDokumen23 halamanMSUDDivya AjithBelum ada peringkat
- English Intervention DialogueDokumen3 halamanEnglish Intervention DialogueJihan Irbah TrianiBelum ada peringkat
- HEPATITIS B VACCINE NURSING RESPONSIBILITIESDokumen14 halamanHEPATITIS B VACCINE NURSING RESPONSIBILITIESJannine BensiBelum ada peringkat
- Amavatha & VathasonithaDokumen125 halamanAmavatha & VathasonithaCicil AbrahamBelum ada peringkat