Anda mungkin juga menyukai
- SC Health and Welfare FormDokumen4 halamanSC Health and Welfare FormLeandro Tamayo14% (7)
- Consent FormDokumen1 halamanConsent FormJun Huan WongBelum ada peringkat
- ICHNT SAR Application FormDokumen4 halamanICHNT SAR Application FormJayBelum ada peringkat
- Patient Access To Medical Records - Request FormDokumen2 halamanPatient Access To Medical Records - Request FormbendeniBelum ada peringkat
- Death Claimant StatementDokumen4 halamanDeath Claimant Statementcet.ranchi7024Belum ada peringkat
- Application FormDokumen2 halamanApplication FormRajat SharmaBelum ada peringkat
- Phillife - Claimant Statement Form - Death ClaimDokumen1 halamanPhillife - Claimant Statement Form - Death ClaimRomeo Ocenar MabutolBelum ada peringkat
- Death Claim Form - Ashx PDFDokumen7 halamanDeath Claim Form - Ashx PDFqaiserjamshedBelum ada peringkat
- Medical AuthorityDokumen2 halamanMedical AuthorityapodhorBelum ada peringkat
- SLOCPI Death Claimant Statement 10may2016 2Dokumen3 halamanSLOCPI Death Claimant Statement 10may2016 2Marc Benedict TalamayanBelum ada peringkat
- Va ReleaseDokumen1 halamanVa Releaseapi-326532936Belum ada peringkat
- Form4 Provisional MMCDokumen3 halamanForm4 Provisional MMCminci sensei100% (2)
- Prisoner Form Medical Mental Health RecordsDokumen3 halamanPrisoner Form Medical Mental Health RecordsMichigan Citizens for Prison ReformBelum ada peringkat
- UntitledDokumen2 halamanUntitledDedik KaryadiBelum ada peringkat
- Annex V InvestigationDokumen2 halamanAnnex V InvestigationGURUDAS PANDITBelum ada peringkat
- Death Claim Checklist 2017Dokumen4 halamanDeath Claim Checklist 2017Cheche GonzalesBelum ada peringkat
- VA - Form - 10-5345 - FillableDokumen2 halamanVA - Form - 10-5345 - Fillablep1nguin0Belum ada peringkat
- Persetujuan RujukanDokumen2 halamanPersetujuan Rujukanmuhammad fahren AliefBelum ada peringkat
- Death Certificate Application and InstructionsDokumen4 halamanDeath Certificate Application and InstructionsMuhammad RaadBelum ada peringkat
- ROMIF - Medika PlazaDokumen1 halamanROMIF - Medika PlazaJemsner Stenly IrothBelum ada peringkat
- FB ScriptDokumen4 halamanFB ScriptDeng SeseBelum ada peringkat
- Request To Access Health InformationDokumen2 halamanRequest To Access Health InformationpkGlobalBelum ada peringkat
- Application For Assistance Under The Supreme Court Health and Welfare Plan (Revised - 2010)Dokumen3 halamanApplication For Assistance Under The Supreme Court Health and Welfare Plan (Revised - 2010)Eunice Navarro100% (1)
- Informed Consent DocumentDokumen1 halamanInformed Consent DocumentDedik KaryadiBelum ada peringkat
- Formulir Death Claim BeneficiaryDokumen4 halamanFormulir Death Claim BeneficiaryHaBelum ada peringkat
- Name of The Deceased (Block Letter)Dokumen2 halamanName of The Deceased (Block Letter)Beyza GemiciBelum ada peringkat
- Death FormDokumen2 halamanDeath FormBeyza GemiciBelum ada peringkat
- Application For Certified Copy of Death Record - vs112Dokumen4 halamanApplication For Certified Copy of Death Record - vs112cylpivkdBelum ada peringkat
- Documents For Marriage Registration in VietnamDokumen9 halamanDocuments For Marriage Registration in VietnamLý Hải YếnBelum ada peringkat
- CGHS Reimbursement FormsDokumen5 halamanCGHS Reimbursement FormsRohit YadavBelum ada peringkat
- Preview Preview: Authorization For Release of Health Information Pursuant To HipaaDokumen2 halamanPreview Preview: Authorization For Release of Health Information Pursuant To HipaaDEShifBelum ada peringkat
- Medical Council RegistrationDokumen4 halamanMedical Council RegistrationAbdul LatheefBelum ada peringkat
- Health Suraksha Claim FormDokumen2 halamanHealth Suraksha Claim FormAnna MalaiBelum ada peringkat
- Sicknessandfitnesscertificates PDFDokumen6 halamanSicknessandfitnesscertificates PDFniraj_sdBelum ada peringkat
- Ssa ReleaseDokumen2 halamanSsa ReleaseMia JacksonBelum ada peringkat
- Hospital StandardQC FormsDokumen22 halamanHospital StandardQC FormstotqmBelum ada peringkat
- MCCD ManualDokumen10 halamanMCCD ManualkalpeshBelum ada peringkat
- Form of Application For Claiming Reimbursement of Medical Expenses of Government Servants and Their FamiliesDokumen5 halamanForm of Application For Claiming Reimbursement of Medical Expenses of Government Servants and Their FamiliesAmit GautamBelum ada peringkat
- Hipaa: Health Insurance Portability and Accountability ActDokumen1 halamanHipaa: Health Insurance Portability and Accountability ActJhoan FrancoBelum ada peringkat
- Hospital Cash ClaimDokumen4 halamanHospital Cash ClaimChloe Auda IbalioBelum ada peringkat
- Provisional RegistrationDokumen9 halamanProvisional RegistrationabuprettyBelum ada peringkat
- Consent Waiver of Medical / Surgery: ST NDDokumen2 halamanConsent Waiver of Medical / Surgery: ST NDrekam medis selaras100% (1)
- Patient Registration Form: A. Demographic InformationDokumen3 halamanPatient Registration Form: A. Demographic Informationyusviyah nurhidayatiBelum ada peringkat
- Patient Access Request - CostcoDokumen1 halamanPatient Access Request - Costcocorey SgarsBelum ada peringkat
- Form-I Donor Application Form Registration No .. (To Be Allotted by The Institution)Dokumen3 halamanForm-I Donor Application Form Registration No .. (To Be Allotted by The Institution)Somashekhara Hulmani75% (4)
- Autopsy Report RequestDokumen1 halamanAutopsy Report RequestshafiraratuBelum ada peringkat
- Affidavit Cert CorrectionDokumen2 halamanAffidavit Cert CorrectionmenergeeBelum ada peringkat
- Advance Medical DirectiveDokumen2 halamanAdvance Medical DirectiveAmisha PrakashBelum ada peringkat
- Access To Health Records Application Form v2Dokumen2 halamanAccess To Health Records Application Form v2Georgie SBelum ada peringkat
- 3288 - Martinez Cintron (Ejemplo-No Completar)Dokumen3 halaman3288 - Martinez Cintron (Ejemplo-No Completar)Eneida Martinez CintronBelum ada peringkat
- Proseguide6 25 13Dokumen18 halamanProseguide6 25 13kbarn389Belum ada peringkat
- Agra DH JhegbcddDokumen20 halamanAgra DH JhegbcddPrdptiwariBelum ada peringkat
- Nomination PaperDokumen1 halamanNomination Paperfelix AdigbliBelum ada peringkat
- ROMIFDokumen2 halamanROMIFChester QuilalaBelum ada peringkat
- Claim FormDokumen4 halamanClaim Formprashant pawarBelum ada peringkat
- Claimant Statement For Credit Life Claims FormDokumen3 halamanClaimant Statement For Credit Life Claims Formsaika tabbasumBelum ada peringkat
- ADNIC Direct Billing Claim Form PDFDokumen2 halamanADNIC Direct Billing Claim Form PDFWilliam IsaacBelum ada peringkat
- Cross-Training: The Medical Assistant WorkbookDari EverandCross-Training: The Medical Assistant WorkbookBelum ada peringkat
- One Step Med: General Medical Information Record Keeping ManualDari EverandOne Step Med: General Medical Information Record Keeping ManualBelum ada peringkat
- Travel Trade Account Executive JDDokumen4 halamanTravel Trade Account Executive JDAnonymous N5Noo7wQFBelum ada peringkat
- SPP Housing Land Supply Statement 2018 PublishedDokumen115 halamanSPP Housing Land Supply Statement 2018 PublishedAnonymous N5Noo7wQFBelum ada peringkat
- Gloucester 20 2016 Runners ExpandedDokumen4 halamanGloucester 20 2016 Runners ExpandedAnonymous N5Noo7wQFBelum ada peringkat
- Highways Newsletter 2016 FebruaryDokumen9 halamanHighways Newsletter 2016 FebruaryAnonymous N5Noo7wQFBelum ada peringkat
- Highways Newsletter 2016 FebruaryDokumen9 halamanHighways Newsletter 2016 FebruaryAnonymous N5Noo7wQFBelum ada peringkat
- Georgian Manor Playhouse Instructions PDFDokumen72 halamanGeorgian Manor Playhouse Instructions PDFAnonymous N5Noo7wQFBelum ada peringkat
- New Wiltshire Council Highway Contract Local Highway ElementDokumen5 halamanNew Wiltshire Council Highway Contract Local Highway ElementAnonymous N5Noo7wQFBelum ada peringkat
- Launch of Parish Steward SchemeDokumen4 halamanLaunch of Parish Steward SchemeAnonymous N5Noo7wQFBelum ada peringkat
- Area Boards Practice PapersDokumen4 halamanArea Boards Practice PapersAnonymous N5Noo7wQFBelum ada peringkat
- New Wiltshire Council Highway Contract Local Highway ElementDokumen5 halamanNew Wiltshire Council Highway Contract Local Highway ElementAnonymous N5Noo7wQFBelum ada peringkat
- Parish Stewards: Denise - Grech@wiltshire - Gov.ukDokumen3 halamanParish Stewards: Denise - Grech@wiltshire - Gov.ukAnonymous N5Noo7wQFBelum ada peringkat
- Highways Newsletter 2016 JuneDokumen3 halamanHighways Newsletter 2016 JuneAnonymous N5Noo7wQFBelum ada peringkat
- Launch of Parish Steward SchemeDokumen4 halamanLaunch of Parish Steward SchemeAnonymous N5Noo7wQFBelum ada peringkat
- Dear Town and Parish Councils I Have Detailed Below Some Points of Special Interest. I Trust This Is of AssistanceDokumen4 halamanDear Town and Parish Councils I Have Detailed Below Some Points of Special Interest. I Trust This Is of AssistanceAnonymous N5Noo7wQFBelum ada peringkat
- Launch of Parish Steward SchemeDokumen4 halamanLaunch of Parish Steward SchemeAnonymous N5Noo7wQFBelum ada peringkat
- Sunday Trading Guidance Notes-2Dokumen2 halamanSunday Trading Guidance Notes-2Anonymous N5Noo7wQFBelum ada peringkat
- Exercise After Stroke Leaflet September 2014Dokumen2 halamanExercise After Stroke Leaflet September 2014Anonymous N5Noo7wQFBelum ada peringkat
- Roles Powers Area Boards Practice PapersDokumen2 halamanRoles Powers Area Boards Practice PapersAnonymous N5Noo7wQFBelum ada peringkat
- Cardiac Phase IV Leaflet September 2014Dokumen2 halamanCardiac Phase IV Leaflet September 2014Anonymous N5Noo7wQFBelum ada peringkat
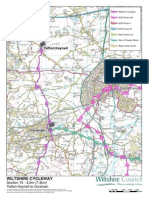
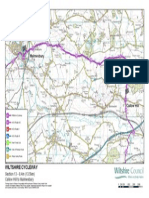
- Wiltshire Cycleway Section10 Great Bedwyn To MarlborougDokumen1 halamanWiltshire Cycleway Section10 Great Bedwyn To MarlborougAnonymous N5Noo7wQFBelum ada peringkat
- Community Asset Transfers Area Boards Practice PapersDokumen4 halamanCommunity Asset Transfers Area Boards Practice PapersAnonymous N5Noo7wQFBelum ada peringkat
- Sunday Trading Guidance Notes-2Dokumen2 halamanSunday Trading Guidance Notes-2Anonymous N5Noo7wQFBelum ada peringkat
- Wiltshire Cycleway Section09 Everleigh To Great BedwynDokumen1 halamanWiltshire Cycleway Section09 Everleigh To Great BedwynAnonymous N5Noo7wQFBelum ada peringkat
- Wiltshire Cycleway Section12 Clyffe Pypard To Callow HiDokumen1 halamanWiltshire Cycleway Section12 Clyffe Pypard To Callow HiAnonymous N5Noo7wQFBelum ada peringkat
- Wiltshire Cycleway Section05 Donhead ST Mary To Broad CDokumen1 halamanWiltshire Cycleway Section05 Donhead ST Mary To Broad CAnonymous N5Noo7wQFBelum ada peringkat
- Wiltshire Cycleway Section16 Corsham To Bradford On AvoDokumen1 halamanWiltshire Cycleway Section16 Corsham To Bradford On AvoAnonymous N5Noo7wQFBelum ada peringkat
- Wiltshire Cycleway Section15 Yatton Keynell To CorshamDokumen1 halamanWiltshire Cycleway Section15 Yatton Keynell To CorshamAnonymous N5Noo7wQFBelum ada peringkat
- Wiltshire Cycleway Section14 Malmesbury To Yatton KeyneDokumen1 halamanWiltshire Cycleway Section14 Malmesbury To Yatton KeyneAnonymous N5Noo7wQFBelum ada peringkat
- Wiltshire Cycleway Section13 Callow Hill To MalmesburyDokumen1 halamanWiltshire Cycleway Section13 Callow Hill To MalmesburyAnonymous N5Noo7wQFBelum ada peringkat
- SafePatientHandling PDFDokumen1 halamanSafePatientHandling PDFdipraBelum ada peringkat
- A Virtual Shopping Task For The Assessment of Executive Functions: Validity For People With StrokeDokumen27 halamanA Virtual Shopping Task For The Assessment of Executive Functions: Validity For People With StrokeMauro GasparofBelum ada peringkat
- Maladaptive Patterns of Behavior Psyche ConceptDokumen273 halamanMaladaptive Patterns of Behavior Psyche Conceptsylphisochi83% (6)
- Unilateral and Bilateral Exercise Movements .6Dokumen7 halamanUnilateral and Bilateral Exercise Movements .6Paula BautistaBelum ada peringkat
- Ayyappan ResumeDokumen5 halamanAyyappan ResumeAyyappan JayavelBelum ada peringkat
- Index2010 BJOTDokumen6 halamanIndex2010 BJOTTO Joss AguilarBelum ada peringkat
- CCrISP 1 IntroductionDokumen19 halamanCCrISP 1 Introductionpioneer92Belum ada peringkat
- Resume 3Dokumen2 halamanResume 3api-548451426Belum ada peringkat
- Skills SurveyDokumen5 halamanSkills Surveyapi-251585548Belum ada peringkat
- Physiotherapy in Neuro Conditions Glady Samuel Raj PDFDokumen331 halamanPhysiotherapy in Neuro Conditions Glady Samuel Raj PDFAnkita Tiwari82% (50)
- OT Interventions To Support Aging in Place RSRDokumen40 halamanOT Interventions To Support Aging in Place RSRNunoBelum ada peringkat
- Bre Online AdvantageDokumen12 halamanBre Online AdvantageKristine SalvoBelum ada peringkat
- Jovel New 27Dokumen42 halamanJovel New 27Anandhu S Prasad0% (1)
- Certificate in Sport Psychology For Athletes DevelopmentDokumen7 halamanCertificate in Sport Psychology For Athletes DevelopmentDragosOlteanBelum ada peringkat
- #8220 Thinking Out of The Box” - From Physiotherapy To RehabilitationDokumen4 halaman#8220 Thinking Out of The Box” - From Physiotherapy To RehabilitationDAriusBelum ada peringkat
- Colgan 2016Dokumen6 halamanColgan 2016Wahyu InsanBelum ada peringkat
- Exercise Therpy 2Dokumen15 halamanExercise Therpy 2Rocky BhaiBelum ada peringkat
- About Cervicogenic Headache .... Imp.Dokumen20 halamanAbout Cervicogenic Headache .... Imp.pervinkumarBelum ada peringkat
- What Do Acute Stroke Physiotherapists Do To Treat Postural Control and MobilityDokumen5 halamanWhat Do Acute Stroke Physiotherapists Do To Treat Postural Control and MobilityAugusto ManoelBelum ada peringkat
- Margie Bissinger, MS, PT, CHC: 6th EditionDokumen31 halamanMargie Bissinger, MS, PT, CHC: 6th EditionAndrea Sirah100% (1)
- Pta Resume ExampleDokumen9 halamanPta Resume Exampleafiwhyber100% (1)
- Sports PhysicalsDokumen18 halamanSports PhysicalsAndika Laksmana Kurniadi100% (1)
- BA BSC Physical Education PDFDokumen15 halamanBA BSC Physical Education PDFRohitBelum ada peringkat
- Evaluation Is Treatment For Low Back PainDokumen11 halamanEvaluation Is Treatment For Low Back PainVizaBelum ada peringkat
- Brukner 3rd Edition - Chapter 1 Clinical Sports MedicineDokumen7 halamanBrukner 3rd Edition - Chapter 1 Clinical Sports MedicineJovana SmoljanićBelum ada peringkat
- Midterm - Examination in Musculoskeletal Physical Therapy For Third Year Students First Semester 2020-2021Dokumen6 halamanMidterm - Examination in Musculoskeletal Physical Therapy For Third Year Students First Semester 2020-2021Dena AliBelum ada peringkat
- CPS Benefits Guide 2014Dokumen29 halamanCPS Benefits Guide 2014Brandon ChavezzBelum ada peringkat
- Master Prgorams-Eligibility Criteria and Fee Structure-2023Dokumen6 halamanMaster Prgorams-Eligibility Criteria and Fee Structure-2023Information InsidserBelum ada peringkat
- Assia CV EngDokumen1 halamanAssia CV Engassia ben yahiaBelum ada peringkat
- CMHNDokumen48 halamanCMHNvikaBelum ada peringkat