Anda mungkin juga menyukai
- Nasalancia Sin FisuraDokumen6 halamanNasalancia Sin FisuraSergio CruzatBelum ada peringkat
- Cephalometric Assessment in OSADokumen10 halamanCephalometric Assessment in OSAAkanksha SrivastavaBelum ada peringkat
- Sataloff 2012Dokumen7 halamanSataloff 2012lakjdlkaBelum ada peringkat
- Sensor I NeuralDokumen3 halamanSensor I NeuralReza AkbarBelum ada peringkat
- Vagal StudyDokumen28 halamanVagal Studyapi-247063958Belum ada peringkat
- VILLA Et Al-2002Dokumen5 halamanVILLA Et Al-2002Naeem MoollaBelum ada peringkat
- Evidence for Etiologies of Adult Sudden Sensorineural Hearing LossDokumen11 halamanEvidence for Etiologies of Adult Sudden Sensorineural Hearing Lossronaldyohanesf87Belum ada peringkat
- Preoperative Characteristics of Over 1,300 Functional Septorhinoplasty PatientsDokumen7 halamanPreoperative Characteristics of Over 1,300 Functional Septorhinoplasty PatientsPablo Segales BautistaBelum ada peringkat
- FulltextDokumen7 halamanFulltextNicolas CruzBelum ada peringkat
- Cephalometric Analysis of Nonobese Snorers Either With or Without Obstructive Sleep Apnea SyndromeDokumen8 halamanCephalometric Analysis of Nonobese Snorers Either With or Without Obstructive Sleep Apnea SyndromeDiego SolaqueBelum ada peringkat
- Asimetrias Atipicas en AutistasDokumen6 halamanAsimetrias Atipicas en AutistasSilvia Pérez FonticiellaBelum ada peringkat
- Vocal analysis of dysarthriasDokumen6 halamanVocal analysis of dysarthriasPriscila Denisse Rodríguez MaunaBelum ada peringkat
- VCS 8Dokumen6 halamanVCS 8Carolina UrrutiaBelum ada peringkat
- Auditory Middle Latency Responses in Individuals With Debilitating TinnitusDokumen7 halamanAuditory Middle Latency Responses in Individuals With Debilitating TinnitusPiyush MalviyaBelum ada peringkat
- Pediatric Laryngopharyngeal Reflux, Perceptual, Acoustic, and Laryngeal T FindingsDokumen5 halamanPediatric Laryngopharyngeal Reflux, Perceptual, Acoustic, and Laryngeal T Findingsarif sudianto100% (1)
- Loge Mann 1978Dokumen11 halamanLoge Mann 1978bencicovakikaBelum ada peringkat
- Lofstrand Articulo FullDokumen11 halamanLofstrand Articulo FullMartin Coronado FalenBelum ada peringkat
- Association of Hearing Impairment With Incident Depressive Symptoms: A Community-Based Prospective StudyDokumen8 halamanAssociation of Hearing Impairment With Incident Depressive Symptoms: A Community-Based Prospective StudyQuentin LISANBelum ada peringkat
- NIH Public Access: Author ManuscriptDokumen14 halamanNIH Public Access: Author ManuscriptamraovcinaBelum ada peringkat
- Minimally Invasive Surgery For The Treatment Of.97204Dokumen7 halamanMinimally Invasive Surgery For The Treatment Of.97204Tamilselvam KakkanaiahBelum ada peringkat
- 2015 Effects of Oropharyngeal Exercises On SnoringDokumen9 halaman2015 Effects of Oropharyngeal Exercises On Snoringjuan pabloBelum ada peringkat
- Dental Causes and Treatments of Deafness, Tinnitus, Vertigo and NeuralgiaDokumen35 halamanDental Causes and Treatments of Deafness, Tinnitus, Vertigo and NeuralgiadcipledudeBelum ada peringkat
- Fulltext02 PDFDokumen28 halamanFulltext02 PDFGabriel CarterBelum ada peringkat
- Laryngeal Computer: by TechniqueDokumen8 halamanLaryngeal Computer: by TechniqueFirda NurmalidaBelum ada peringkat
- X-Rays in The Evaluation of Adenoid Hypertrophy: It'S Role in The Endoscopic EraDokumen3 halamanX-Rays in The Evaluation of Adenoid Hypertrophy: It'S Role in The Endoscopic EraDr.M.H. PatelBelum ada peringkat
- Laryngopharyngeal Reflux and Voice DisordersDokumen20 halamanLaryngopharyngeal Reflux and Voice DisordersDiana RodriguezBelum ada peringkat
- Multi-Site Diagnosis and Management of 260 Patients With Auditory Neuropathy - Dys-Synchrony (Auditory Neuropathy Spectrum Disorder)Dokumen15 halamanMulti-Site Diagnosis and Management of 260 Patients With Auditory Neuropathy - Dys-Synchrony (Auditory Neuropathy Spectrum Disorder)Ailin TosiBelum ada peringkat
- The Utility of Pitch Elevation in the Evaluation of Oropharyngeal Dysphagia- Preliminary FindingsDokumen8 halamanThe Utility of Pitch Elevation in the Evaluation of Oropharyngeal Dysphagia- Preliminary FindingsESTEFANIA GEOVANNA MEJIA MACASBelum ada peringkat
- Apneia Obstrutiva Do Sono em Mulheres Estudo Da Fala e Características Craniofaciais - TCC E IcDokumen17 halamanApneia Obstrutiva Do Sono em Mulheres Estudo Da Fala e Características Craniofaciais - TCC E IcRichard Lima OficialBelum ada peringkat
- Measuring Severity of Tinnitus With A Visual Analog ScaleDokumen4 halamanMeasuring Severity of Tinnitus With A Visual Analog ScaleCamiloBelum ada peringkat
- Audiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The LiteratureDokumen12 halamanAudiologic Management of AuditoryNeuropathy Spectrum Disorder in ChildrenA Systematic Review of The Literaturericardorojas2403Belum ada peringkat
- Otology: Special Paper in Celebration of Prof. Yang'S 50 Years Career in MedicineDokumen6 halamanOtology: Special Paper in Celebration of Prof. Yang'S 50 Years Career in Medicinechipta lestariBelum ada peringkat
- Demetriades 2010Dokumen6 halamanDemetriades 2010Sai Rakesh ChavaBelum ada peringkat
- Audioanalgesia As An Adjunct To Mobilization of The Chronic Frozen ShoulderDokumen8 halamanAudioanalgesia As An Adjunct To Mobilization of The Chronic Frozen ShoulderIntan Eddy ParindinganBelum ada peringkat
- Schwannoma Vestibular TinnitusDokumen6 halamanSchwannoma Vestibular TinnitusThomasMáximoMancinelliRinaldoBelum ada peringkat
- Disfuncion de Cuedas VocalesDokumen6 halamanDisfuncion de Cuedas VocalesJan SaldañaBelum ada peringkat
- Mezze Dim I 2016Dokumen8 halamanMezze Dim I 2016Marcos ChuquiagoBelum ada peringkat
- Articulo Disartria y Paralisis CerebralDokumen6 halamanArticulo Disartria y Paralisis CerebralHaizea MuñozBelum ada peringkat
- Nasolaryngoscopy in A Family Medicine Clinic: Indications, Findings, and EconomicsDokumen7 halamanNasolaryngoscopy in A Family Medicine Clinic: Indications, Findings, and Economicsriski novitaBelum ada peringkat
- Academic Emergency Medicine - 2011 - Adhikari - Pilot Study To Determine The Utility of Point of Care Ultrasound in TheDokumen7 halamanAcademic Emergency Medicine - 2011 - Adhikari - Pilot Study To Determine The Utility of Point of Care Ultrasound in TheIndhu SubbuBelum ada peringkat
- Tinnitus Today November 1981 Vol 6, No 3Dokumen4 halamanTinnitus Today November 1981 Vol 6, No 3American Tinnitus AssociationBelum ada peringkat
- Craniofacial and Upper Airway Morphology inDokumen14 halamanCraniofacial and Upper Airway Morphology inkerminkBelum ada peringkat
- Do musicians sleep well? A review of wind playing and singing on sleep apnea riskDokumen11 halamanDo musicians sleep well? A review of wind playing and singing on sleep apnea riskFawn100% (1)
- ASSR Thresholds PDFDokumen7 halamanASSR Thresholds PDFDaniela Garrido GonzálezBelum ada peringkat
- Association Between Posture Voice Dysphonia ReviewDokumen12 halamanAssociation Between Posture Voice Dysphonia ReviewChristaire AfariBelum ada peringkat
- Ann Clin Transl Neurol - 2019 - Campbell - Hearing Impairment After Subarachnoid HemorrhageDokumen11 halamanAnn Clin Transl Neurol - 2019 - Campbell - Hearing Impairment After Subarachnoid HemorrhageChavdarBelum ada peringkat
- NUNES en V75n2a06Dokumen5 halamanNUNES en V75n2a06Anonymous Qr9nZRbBelum ada peringkat
- A Nomenclature Paradigm For Benign Midmembranous Vocal Fold LesionsDokumen7 halamanA Nomenclature Paradigm For Benign Midmembranous Vocal Fold Lesionsnatalia.gallinoBelum ada peringkat
- Vocal Function Exercises For Presbylaryn PDFDokumen9 halamanVocal Function Exercises For Presbylaryn PDFAngela Lleuful ToledoBelum ada peringkat
- 26-34 OTO 4 2018 Hojna AngDokumen9 halaman26-34 OTO 4 2018 Hojna AngcpaladinestBelum ada peringkat
- Zobay Et Al 2023 Fitting A Hearing Aid On The Better Ear Worse Ear or Both Associations of Hearing Aid FittingDokumen13 halamanZobay Et Al 2023 Fitting A Hearing Aid On The Better Ear Worse Ear or Both Associations of Hearing Aid FittingAlex A.Belum ada peringkat
- Vocal Function Exercises For Presbylaryngis: A Multidimensional Assessment of Treatment OutcomesDokumen10 halamanVocal Function Exercises For Presbylaryngis: A Multidimensional Assessment of Treatment OutcomesJulia GavrashenkoBelum ada peringkat
- Clinical characteristics of mutational dysphoniaDokumen8 halamanClinical characteristics of mutational dysphoniamariola_joplinBelum ada peringkat
- Wang 1995 Sonographic Lenticulostriate Vasculopathy in InfantsDokumen11 halamanWang 1995 Sonographic Lenticulostriate Vasculopathy in InfantsModou NianeBelum ada peringkat
- TREP12Dokumen10 halamanTREP12Chiều Biển VắngBelum ada peringkat
- Velopharyngeal InsufficiencyDokumen9 halamanVelopharyngeal InsufficiencyJASPREETKAUR0410Belum ada peringkat
- Audiology and Familial Adenomatous Polyposis: Do You Hear What I Hear?Dokumen1 halamanAudiology and Familial Adenomatous Polyposis: Do You Hear What I Hear?Harshit AmbeshBelum ada peringkat
- Am J Otolaryngol: Eugene Hung Chih Wong, Aun Wee ChongDokumen5 halamanAm J Otolaryngol: Eugene Hung Chih Wong, Aun Wee ChongLee제노Belum ada peringkat
- Fatigue and perfectionism in functional dysphoniaDokumen6 halamanFatigue and perfectionism in functional dysphoniaMuhamad AriefBelum ada peringkat
- Evidence-Based LaryngologyDari EverandEvidence-Based LaryngologyDavid E. RosowBelum ada peringkat
- Escala Disconfort TractoDokumen7 halamanEscala Disconfort Tractofono2013Belum ada peringkat
- A Case Report in Changes in Phonatory Physiology Following Voice TherapyDokumen8 halamanA Case Report in Changes in Phonatory Physiology Following Voice Therapyfono2013Belum ada peringkat
- The Performer's Voice Capitulo 7Dokumen16 halamanThe Performer's Voice Capitulo 7fono2013Belum ada peringkat
- 2 Pattern Recognition in Muscle Misuse Voice Disorders - How To Do ItDokumen7 halaman2 Pattern Recognition in Muscle Misuse Voice Disorders - How To Do Itfono2013Belum ada peringkat
- PlanoDokumen1 halamanPlanofono2013Belum ada peringkat
- Lecture 1 EpidemiologyDokumen7 halamanLecture 1 EpidemiologyWael Lotfy0% (1)
- Anti-HSV-2 IgG Herpes Simplex Virus Type 2Dokumen2 halamanAnti-HSV-2 IgG Herpes Simplex Virus Type 2ElenaBelum ada peringkat
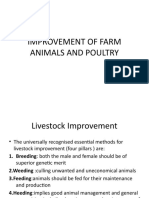
- Student Copy LIVESTOCK AND POULTRY MANAGEMENT - IIDokumen162 halamanStudent Copy LIVESTOCK AND POULTRY MANAGEMENT - IIBhàvyà Shréé ÆgríBelum ada peringkat
- Block 4 Lung PathDokumen31 halamanBlock 4 Lung PathShalini ShanmugalingamBelum ada peringkat
- 2005 Coxe Cooper Avian FluDokumen37 halaman2005 Coxe Cooper Avian Flupep59Belum ada peringkat
- Case-Urinary Catheterizarion DR - PNTDokumen38 halamanCase-Urinary Catheterizarion DR - PNTWan Adi OeyaBelum ada peringkat
- Akapulko or Acapulco in English Is A Shrub Found Throughout The PhilippinesDokumen8 halamanAkapulko or Acapulco in English Is A Shrub Found Throughout The Philippinesmuskeeto100% (4)
- 01 Public Health NursingDokumen20 halaman01 Public Health NursingKailash NagarBelum ada peringkat
- 15 - Chapter 7 PDFDokumen4 halaman15 - Chapter 7 PDFRamBelum ada peringkat
- Coronavirus Depopulation Agenda Exposed by Ex-Russian Intel OfficerDokumen9 halamanCoronavirus Depopulation Agenda Exposed by Ex-Russian Intel OfficerAlison ABelum ada peringkat
- Scribd Chapters 156628Dokumen188 halamanScribd Chapters 156628inkpopBelum ada peringkat
- LAS #2 - Frayer ModelDokumen4 halamanLAS #2 - Frayer ModelLexia J. BautistaBelum ada peringkat
- 10 Children's Charities To SupportDokumen8 halaman10 Children's Charities To SupportAvegail TolentinoBelum ada peringkat
- Portfolio Clinical Case Study 3 Lymphoma FinalDokumen27 halamanPortfolio Clinical Case Study 3 Lymphoma Finalapi-277136509Belum ada peringkat
- COMPLAINT Against All Defendants, Filed by Patricia Brantley, Grace Straney, Grace KinardDokumen33 halamanCOMPLAINT Against All Defendants, Filed by Patricia Brantley, Grace Straney, Grace KinardABC15 NewsBelum ada peringkat
- History of Navy Entomology 1941-2011Dokumen35 halamanHistory of Navy Entomology 1941-2011rville1559Belum ada peringkat
- Case Report SleDokumen37 halamanCase Report SleUswah SudirmanBelum ada peringkat
- Ards and RF FileDokumen12 halamanArds and RF FileEdwin Delos Reyes Abu100% (1)
- Parts of The Human Eye With DefinitionDokumen4 halamanParts of The Human Eye With DefinitionStarsky Allence Puyoc0% (1)
- Luxury Travel Rebound as 52% Plan 2021 TripsDokumen8 halamanLuxury Travel Rebound as 52% Plan 2021 TripsAshu SinghBelum ada peringkat
- Thesis Jessica KattanDokumen45 halamanThesis Jessica Kattanaztigan100% (2)
- Life PrinciplesDokumen2 halamanLife PrinciplesBorja Verlene Jessamine RosalesBelum ada peringkat
- Contact Lens Complications and ManagementDokumen10 halamanContact Lens Complications and Managementstrawberry8832850% (2)
- 2.1 Philippine History of MedicineDokumen17 halaman2.1 Philippine History of Medicinejessica callBelum ada peringkat
- DOH authority to declare quarantine without local transmissionDokumen2 halamanDOH authority to declare quarantine without local transmissionJoni AquinoBelum ada peringkat
- Operative Dentistry: Patient Evaluation, Diagnosis and Treatment PlanningDokumen5 halamanOperative Dentistry: Patient Evaluation, Diagnosis and Treatment PlanningMohammed100% (1)
- Filariasis: Signs and SymptomsDokumen30 halamanFilariasis: Signs and SymptomsAnonymous VJjzqbAlBelum ada peringkat
- Pamplet - English PDFDokumen4 halamanPamplet - English PDF9884288233100% (1)
- Tumors and Syndromes of the Oral CavityDokumen23 halamanTumors and Syndromes of the Oral CavityAsma Sam100% (3)
- Poultry FarmingDokumen11 halamanPoultry FarmingbimalBelum ada peringkat