Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- An Introduction Into The Misuse of Drugs ActDokumen26 halamanAn Introduction Into The Misuse of Drugs Actkalli987Belum ada peringkat
- Sodium Nitrite BASFDokumen4 halamanSodium Nitrite BASFPanos AnastasiadisBelum ada peringkat
- Penulisan Resep Yang Baik Dan BenarDokumen2 halamanPenulisan Resep Yang Baik Dan BenarEdward KurniawanBelum ada peringkat
- Medical and Pharmaceutical Commoditi 4 C 8 GRDokumen1 halamanMedical and Pharmaceutical Commoditi 4 C 8 GROksanaBelum ada peringkat
- Antituberculosis DrugsDokumen30 halamanAntituberculosis DrugsI Kadek Adi Putra Suandana 2005Belum ada peringkat
- Juris NepalDokumen8 halamanJuris NepalAmrit GaireBelum ada peringkat
- Handbook On Herbal Products (Medicines, Cosmetics, Toiletries, Perfumes) 2 Vols. - Chapter 'Herbal Cosmetics'Dokumen41 halamanHandbook On Herbal Products (Medicines, Cosmetics, Toiletries, Perfumes) 2 Vols. - Chapter 'Herbal Cosmetics'randatagBelum ada peringkat
- Clientes Farmovet 16-11Dokumen4 halamanClientes Farmovet 16-11Christian Alejandro BarretoBelum ada peringkat
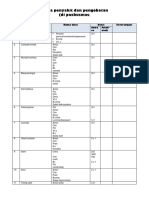
- Obat PuskesmasDokumen14 halamanObat PuskesmassusiBelum ada peringkat
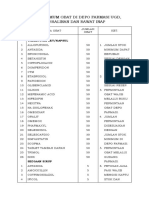
- Stok Minimum Obat Di Depo Farmasi Ugd, Persalinan Dan Rawat InapDokumen2 halamanStok Minimum Obat Di Depo Farmasi Ugd, Persalinan Dan Rawat InapsumalataBelum ada peringkat
- Pharmacology - Principles and Applications, 3rd EditionDokumen657 halamanPharmacology - Principles and Applications, 3rd Editionserenesh67% (3)
- Nutra World ArticleDokumen5 halamanNutra World ArticleAki EspaldonBelum ada peringkat
- ZeronaDokumen2 halamanZeronaAlex ShparberBelum ada peringkat
- Insecticide BasicsDokumen8 halamanInsecticide Basicsrotsacreijav666666Belum ada peringkat
- Rahul Krishna Pandharpatte-3Dokumen3 halamanRahul Krishna Pandharpatte-3Vidhya ChuriBelum ada peringkat
- Pharmacokinetics Cephalexin: Dosage Nomograms Impaired: of Cefaclor and For Renal FunctionDokumen6 halamanPharmacokinetics Cephalexin: Dosage Nomograms Impaired: of Cefaclor and For Renal FunctionnofiasaridBelum ada peringkat
- Industrial Pharmacy: Role of Pharmacy and The Philippine Drug IndustryDokumen9 halamanIndustrial Pharmacy: Role of Pharmacy and The Philippine Drug IndustrycherrykuraBelum ada peringkat
- Unicom Chemist Limited: SG PharmaDokumen10 halamanUnicom Chemist Limited: SG PharmaImanoelClousAndohBelum ada peringkat
- MNCGeneric US 11172020Dokumen6 halamanMNCGeneric US 11172020Er GaBelum ada peringkat
- DischargeDokumen49 halamanDischargejonel_amarilleBelum ada peringkat
- Managing Drug Suply 2017.Ppt AZIZAHDokumen17 halamanManaging Drug Suply 2017.Ppt AZIZAHwandameritaBelum ada peringkat
- Comparative Pharmacokinetics of Rhein in Normal and Loperam 2014 Journal ofDokumen9 halamanComparative Pharmacokinetics of Rhein in Normal and Loperam 2014 Journal ofcds_tolucaBelum ada peringkat
- Kokristal ParasetamolDokumen6 halamanKokristal Parasetamolslmkhns46Belum ada peringkat
- 2018 AGS Beers Criteria - For Review Period 8.13.18 PDFDokumen53 halaman2018 AGS Beers Criteria - For Review Period 8.13.18 PDFDarmawatyMalikBelum ada peringkat
- Pharmacokinetics and Dose Selection of A Novel, Long-Acting Transdermal Fentanyl Solution in Healthy Laboratory BeaglesDokumen6 halamanPharmacokinetics and Dose Selection of A Novel, Long-Acting Transdermal Fentanyl Solution in Healthy Laboratory BeaglesRhanna AbreuBelum ada peringkat
- Becky ReportDokumen4 halamanBecky ReportAnonymous mJ9GLjN5eaBelum ada peringkat
- Bioassay: Satish Kumar.J PH.D Student Mysore UniversityDokumen21 halamanBioassay: Satish Kumar.J PH.D Student Mysore UniversityaziskfBelum ada peringkat
- PiroxicamDokumen10 halamanPiroxicamPapaindoBelum ada peringkat
- Systemic Enzyme TherapyDokumen10 halamanSystemic Enzyme TherapyAndrei GabrielBelum ada peringkat
- Draft of Volume 9a 12 2005 enDokumen198 halamanDraft of Volume 9a 12 2005 englobalpharmatek100% (1)