Anda mungkin juga menyukai
- 5550 FullDokumen8 halaman5550 FulldupuytrenBelum ada peringkat
- Nonviral Polymeric Nanoparticles For Gene Therapy in Pediatric CNS MalignanciesDokumen31 halamanNonviral Polymeric Nanoparticles For Gene Therapy in Pediatric CNS MalignanciesNisargaBelum ada peringkat
- NeuroblastomaDokumen19 halamanNeuroblastomaTri Andhika Dessy WahyuniBelum ada peringkat
- 1 Neurosurgery Cases and ReviewsDokumen5 halaman1 Neurosurgery Cases and ReviewsintodoieblissBelum ada peringkat
- Embryonal CnsDokumen13 halamanEmbryonal CnsPoly EdayanalBelum ada peringkat
- New WHO Classification of Pituitary Adenomas (4th Edition) : Assessment of Pituitary Transcription Factors and The Prognostic Histological FactorsDokumen5 halamanNew WHO Classification of Pituitary Adenomas (4th Edition) : Assessment of Pituitary Transcription Factors and The Prognostic Histological FactorscristianescBelum ada peringkat
- Flucke 2013Dokumen8 halamanFlucke 2013FANIA PARRABelum ada peringkat
- Neuroendocrine Tumors: Surgical Evaluation and ManagementDari EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydBelum ada peringkat
- Oncovet 2008Dokumen18 halamanOncovet 2008Frederico VelascoBelum ada peringkat
- RPB14150079015Dokumen5 halamanRPB14150079015Ijupbs IjupbsBelum ada peringkat
- Pathological Pattern of Atypical Meningioma-Diagnostic Criteria and Tumor Recurrence Predictors by Mohamed A.R ArbabDokumen8 halamanPathological Pattern of Atypical Meningioma-Diagnostic Criteria and Tumor Recurrence Predictors by Mohamed A.R Arbabijr_journalBelum ada peringkat
- Braf DiaDokumen15 halamanBraf DiaNadir KoçakBelum ada peringkat
- Small Round Cells of Head and NeckDokumen10 halamanSmall Round Cells of Head and NeckBlazxy EyreBelum ada peringkat
- Stem Cells and Cancer Stem Cells, Volume 3 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 3Dokumen426 halamanStem Cells and Cancer Stem Cells, Volume 3 - Stem Cells and Cancer Stem Cells, Therapeutic Applications in Disease and Injury - Volume 3Artan100% (1)
- Common Musculoskeletal Tumors of ChildhoodDokumen13 halamanCommon Musculoskeletal Tumors of ChildhoodMari CherBelum ada peringkat
- Jurnal Sitologi PDFDokumen5 halamanJurnal Sitologi PDFIbnu Satria ApriansaBelum ada peringkat
- Review Article: Recent Advances in Childhood Brain TumoursDokumen10 halamanReview Article: Recent Advances in Childhood Brain Tumoursjosue_wigBelum ada peringkat
- Atypical Pituitary Adenoma: A Case ReportDokumen3 halamanAtypical Pituitary Adenoma: A Case ReportMuhammad Hafizh Islam SadidaBelum ada peringkat
- Characteristics and Outcome of Patients With Ganglioneuroblastoma, Nodular Subtype: A Report From The INRG ProjectDokumen7 halamanCharacteristics and Outcome of Patients With Ganglioneuroblastoma, Nodular Subtype: A Report From The INRG ProjectWahyudhy SajaBelum ada peringkat
- Kim 2017Dokumen14 halamanKim 2017Cota AncutaBelum ada peringkat
- As Trocito MaDokumen10 halamanAs Trocito Majeimy_carolina4163Belum ada peringkat
- Brain Tumors in ChildrenDari EverandBrain Tumors in ChildrenAmar GajjarBelum ada peringkat
- Accuracy of Computerised Tomography in Diagnosis of Brain Tumours in ChildrenDokumen3 halamanAccuracy of Computerised Tomography in Diagnosis of Brain Tumours in ChildrenVidinikusumaBelum ada peringkat
- ClinicalCharacteristicsAndProgrognostic AstrocytomaDokumen12 halamanClinicalCharacteristicsAndProgrognostic AstrocytomaDesty PurnamasariBelum ada peringkat
- SWAIMANDokumen18 halamanSWAIMANVan John MagallanesBelum ada peringkat
- Askin's TumorDokumen5 halamanAskin's Tumoranon_828221297Belum ada peringkat
- Diagnostic and Prognostic Markers For Gastrointestinal Stromal Tumors in NorwayDokumen8 halamanDiagnostic and Prognostic Markers For Gastrointestinal Stromal Tumors in NorwayNengLukmanBelum ada peringkat
- Cpho023 01 03Dokumen11 halamanCpho023 01 03Kyung-Nam KohBelum ada peringkat
- Prognostic Implications of PD-L1 Expression in Patients With Soft Tissue SarcomaDokumen7 halamanPrognostic Implications of PD-L1 Expression in Patients With Soft Tissue SarcomaJemma ArakelyanBelum ada peringkat
- Cpho023 02 07Dokumen9 halamanCpho023 02 07Kyung-Nam KohBelum ada peringkat
- Pathologic Quiz Case: Ovarian Mass in A 2-Year-Old Girl Presenting With Pleural EffusionsDokumen4 halamanPathologic Quiz Case: Ovarian Mass in A 2-Year-Old Girl Presenting With Pleural EffusionsMateen ShukriBelum ada peringkat
- Modpathol 201783Dokumen14 halamanModpathol 201783Tian Nopita SariBelum ada peringkat
- Adrenal Neuroblastoma With Bone Marrow Metastasis in Anadult: A Case Report and Review of The LiteratureDokumen5 halamanAdrenal Neuroblastoma With Bone Marrow Metastasis in Anadult: A Case Report and Review of The LiteratureIJAR JOURNALBelum ada peringkat
- 2012 Published OC GL Radionuclide Imaging of Phaeochromocytoma and ParagangliomaDokumen19 halaman2012 Published OC GL Radionuclide Imaging of Phaeochromocytoma and ParagangliomaLadipo Temitope AyodejiBelum ada peringkat
- Ref 14Dokumen8 halamanRef 14Tiago BaraBelum ada peringkat
- Immunohistochemistry in Undifferentiated Neoplasm/Tumor of Uncertain OriginDokumen28 halamanImmunohistochemistry in Undifferentiated Neoplasm/Tumor of Uncertain OriginLaura BratulescuBelum ada peringkat
- Pediatric Acute Lymphoblastic LeukemiaDari EverandPediatric Acute Lymphoblastic LeukemiaMotohiro KatoBelum ada peringkat
- Mri Evaluation of Medulloblastoma With Histopahtological CorrelationDokumen5 halamanMri Evaluation of Medulloblastoma With Histopahtological CorrelationVidinikusumaBelum ada peringkat
- Shi 2017Dokumen8 halamanShi 2017Claudia Ivette Villarreal OvalleBelum ada peringkat
- Fine Needle Aspiration Cytology (FNAC) of GISTDokumen7 halamanFine Needle Aspiration Cytology (FNAC) of GISTurfriendanshul100% (1)
- Jkns 57 315Dokumen8 halamanJkns 57 315arcobaleno589Belum ada peringkat
- Small Round Cell Tumors of Soft Tissue and BoneDokumen13 halamanSmall Round Cell Tumors of Soft Tissue and BoneAdriana Gabriela Ugarte MacíasBelum ada peringkat
- Metaplastic CA 2 IhkDokumen10 halamanMetaplastic CA 2 IhkWinta MayantiBelum ada peringkat
- Parkinsons TreatmeantDokumen7 halamanParkinsons Treatmeantkhadija khokhawalaBelum ada peringkat
- Neonatal Brain Tumors A Review 2017Dokumen5 halamanNeonatal Brain Tumors A Review 2017FarhanBelum ada peringkat
- ECP 2017 Asbtracts Supplement (12 Lucrari)Dokumen14 halamanECP 2017 Asbtracts Supplement (12 Lucrari)Cristiana PoppBelum ada peringkat
- Pediatri RabdomyosarkomDokumen7 halamanPediatri RabdomyosarkomDogukan DemirBelum ada peringkat
- Non Small-Cell Lung Cancer in A 15-Year-Old NonsmokerDokumen2 halamanNon Small-Cell Lung Cancer in A 15-Year-Old Nonsmokertonirian99Belum ada peringkat
- Benitez-Ribas 2018Dokumen9 halamanBenitez-Ribas 2018docadax848Belum ada peringkat
- Anaplastic Sarcoma of The Kidney With Chromosomal AbnormalityDokumen5 halamanAnaplastic Sarcoma of The Kidney With Chromosomal AbnormalityJose Alejandro InciongBelum ada peringkat
- NeuroblastomaDokumen9 halamanNeuroblastomasamantha mccoyBelum ada peringkat
- Abdollahi Et AlDokumen5 halamanAbdollahi Et AlMarc DaouBelum ada peringkat
- Prognostic Significance of PINCH Signalling in Human Pancreatic Ductal AdenocarcinomaDokumen7 halamanPrognostic Significance of PINCH Signalling in Human Pancreatic Ductal AdenocarcinomaLuis FuentesBelum ada peringkat
- Cytoplasmic Maspin Expression Predicts Poor Prognosis of Patients With Soft Tissue SarcomasDokumen7 halamanCytoplasmic Maspin Expression Predicts Poor Prognosis of Patients With Soft Tissue SarcomasAndreea RelenschiBelum ada peringkat
- Translational Research in Breast CancerDari EverandTranslational Research in Breast CancerDong-Young NohBelum ada peringkat
- Astrocytoma 10.1007/s00401-015-1410-7Dokumen14 halamanAstrocytoma 10.1007/s00401-015-1410-7Rikizu HobbiesBelum ada peringkat
- Brain Tumor Thesis StatementDokumen8 halamanBrain Tumor Thesis Statementchristinamartinspringfield100% (2)
- Ijohns 2015083115062935 PDFDokumen6 halamanIjohns 2015083115062935 PDFradifBelum ada peringkat
- Primaey Neolplasm of The LungDokumen8 halamanPrimaey Neolplasm of The Lungsamuel kefyalewBelum ada peringkat
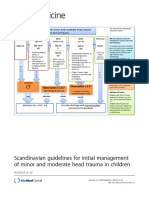
- Scandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenDokumen20 halamanScandinavian Guidelines For Initial Management of Minor and Moderate Head Trauma in ChildrenRafael Mujica OreBelum ada peringkat
- Giant AneurysmDokumen11 halamanGiant AneurysmRafael Mujica OreBelum ada peringkat
- Madsen 2013Dokumen7 halamanMadsen 2013Rafael Mujica OreBelum ada peringkat
- 10 1002@jso 25178 PDFDokumen11 halaman10 1002@jso 25178 PDFRafael Mujica OreBelum ada peringkat
- Neurocytoma/rhabdomyoma (Myoneurocytoma) of The CerebellumDokumen6 halamanNeurocytoma/rhabdomyoma (Myoneurocytoma) of The CerebellumRafael Mujica OreBelum ada peringkat
- Prokaryote Vs Eukaryote WorksheetDokumen2 halamanProkaryote Vs Eukaryote WorksheetAra Hella JordasBelum ada peringkat
- Radiobiology Lecture 3 Cellular EffectsDokumen29 halamanRadiobiology Lecture 3 Cellular EffectsMankit LoBelum ada peringkat
- General Sciece PRTDokumen98 halamanGeneral Sciece PRTChaudhary ChitizBelum ada peringkat
- Evolution of EukaryotesDokumen25 halamanEvolution of EukaryotesCharleneKronstedtBelum ada peringkat
- Las q3 Week-2 Gen - Bio-1 Viros SnsDokumen10 halamanLas q3 Week-2 Gen - Bio-1 Viros SnsFranzhean Balais CuachonBelum ada peringkat
- Detailed Lesson Plan in Science 7Dokumen11 halamanDetailed Lesson Plan in Science 7Anton Orbon100% (4)
- Bio Unit 2Dokumen25 halamanBio Unit 2benlucag5Belum ada peringkat
- Principles Of: BiochemistryDokumen52 halamanPrinciples Of: BiochemistryShaden MasriBelum ada peringkat
- Effectiveness of The Utilization of Strategic Intervention Material FinaleDokumen27 halamanEffectiveness of The Utilization of Strategic Intervention Material Finalelelibeth curada100% (1)
- Prokaryotic Vs Eukaryotic Cells: Shs Stem - Biology 1Dokumen17 halamanProkaryotic Vs Eukaryotic Cells: Shs Stem - Biology 1Dette Dominic BallanoBelum ada peringkat
- MSC MPlil ZoologyDokumen18 halamanMSC MPlil ZoologyYougesh KumarBelum ada peringkat
- EBIO-Table On Chromosomal Abnormalities-1Dokumen2 halamanEBIO-Table On Chromosomal Abnormalities-1Alyanna Elisse VergaraBelum ada peringkat
- Cell NotesDokumen12 halamanCell NotesP1Belum ada peringkat
- Leapotswe International School: Cambridge IGCSEDokumen16 halamanLeapotswe International School: Cambridge IGCSEShepherd W NgwenyaBelum ada peringkat
- CellStructureSEDokumen3 halamanCellStructureSEJin KingBelum ada peringkat
- Answers - Worksheet - 8th - Science - 2021-10-02T02:27Dokumen17 halamanAnswers - Worksheet - 8th - Science - 2021-10-02T02:27omsudhirBelum ada peringkat
- Special ChromosomesDokumen68 halamanSpecial ChromosomesRashmi AshokBelum ada peringkat
- Human Heredity Principles and Issues 11th Edition Cummings Solution ManualDokumen56 halamanHuman Heredity Principles and Issues 11th Edition Cummings Solution Manualmichael100% (21)
- Genbio ReviewerDokumen7 halamanGenbio ReviewerMary Jean BoBelum ada peringkat
- Biology Study Guide 7Dokumen66 halamanBiology Study Guide 7api-418176886Belum ada peringkat
- Grade 9 Science (10F) : A Course For Independent StudyDokumen40 halamanGrade 9 Science (10F) : A Course For Independent StudyRF Liao Sabado100% (1)
- Making of A Fly, The - Lawrence, Peter ADokumen243 halamanMaking of A Fly, The - Lawrence, Peter ADương Minh ĐứcBelum ada peringkat
- 9700 Y16 Sy 1Dokumen81 halaman9700 Y16 Sy 1api-255467062Belum ada peringkat
- Human Molecular Genetics, 4th Edition PDFDokumen704 halamanHuman Molecular Genetics, 4th Edition PDFLi Luo100% (5)
- 1C-Tabugoc - LA2 Plant CellDokumen5 halaman1C-Tabugoc - LA2 Plant CellClint Jhun TabugocBelum ada peringkat
- Genbio 1 1ST Grading ReviewerDokumen11 halamanGenbio 1 1ST Grading ReviewerTodo Roki100% (1)
- Cell Cycle and Mitosis Webquest Cells AliveDokumen4 halamanCell Cycle and Mitosis Webquest Cells AliveBraedyn JohnsonBelum ada peringkat
- Glioma - Chinh SuaDokumen176 halamanGlioma - Chinh SuaHikari AoiBelum ada peringkat
- Life Science Basics For The GEDDokumen6 halamanLife Science Basics For The GEDPinn phaBelum ada peringkat
- A2AS BIOL Specification 2008 1270Dokumen95 halamanA2AS BIOL Specification 2008 1270Naledi TadiwaBelum ada peringkat