Anda mungkin juga menyukai
- VasopressinDokumen2 halamanVasopressinKim LompotBelum ada peringkat
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- DiureticsDokumen4 halamanDiureticsNazmul Islam AbirBelum ada peringkat
- DiureticsDokumen4 halamanDiureticsdhainey100% (3)
- Pharmacology Chart 3Dokumen2 halamanPharmacology Chart 3Omar ClorBelum ada peringkat
- Endocrine Drug ChartDokumen1 halamanEndocrine Drug ChartJessicaBelum ada peringkat
- PHARMACOLOGY Anti Microbial DrugsDokumen17 halamanPHARMACOLOGY Anti Microbial DrugsLeilani Sablan100% (2)
- Diuretic Drugs For Nursing PharmacologyDokumen1 halamanDiuretic Drugs For Nursing Pharmacologylhayes1234100% (7)
- Drug Outline: Autonomic Nervous System Drug Class Drug OtherDokumen4 halamanDrug Outline: Autonomic Nervous System Drug Class Drug OtherCess Lagera YbanezBelum ada peringkat
- Medsurg Test 4Dokumen11 halamanMedsurg Test 4Tori RolandBelum ada peringkat
- Anticoagulants Drug TableDokumen1 halamanAnticoagulants Drug Tablecdp158767% (3)
- Complete Drug GuideDokumen225 halamanComplete Drug GuideJessica 'Baker' IsaacsBelum ada peringkat
- Hematology QuestionsDokumen7 halamanHematology QuestionsRaven Atisha100% (1)
- Pharmacology FirecrackerDokumen37 halamanPharmacology FirecrackerRehan Usman100% (1)
- Musculoskeletal PharmacologyDokumen18 halamanMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Autonomic DrugsDokumen107 halamanAutonomic DrugsMaria Mercedes LeivaBelum ada peringkat
- Anti Hypertensive Drugs - DiureticsDokumen49 halamanAnti Hypertensive Drugs - DiureticsApurba Sarker Apu100% (1)
- Drugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteDokumen2 halamanDrugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteyukariBelum ada peringkat
- Anemia: Ch. 31 Hematologic ProblemsDokumen36 halamanAnemia: Ch. 31 Hematologic Problemshops23100% (3)
- Cancer DrugsDokumen5 halamanCancer DrugsLinh HoangBelum ada peringkat
- GI MnemonicsDokumen14 halamanGI Mnemonicsjonnyahn100% (1)
- Bumetanide Torsemide: Desmopressin - V2Dokumen1 halamanBumetanide Torsemide: Desmopressin - V2med testBelum ada peringkat
- Renal Excretion of DrugsDokumen3 halamanRenal Excretion of DrugsGerardLum100% (3)
- Review Handouts For Medical Pharmacology PDFDokumen21 halamanReview Handouts For Medical Pharmacology PDFAndres F. TorresBelum ada peringkat
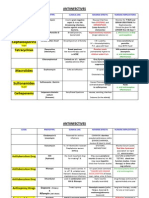
- Antiinfectives Drug TableDokumen5 halamanAntiinfectives Drug Tablecdp1587100% (3)
- Classification of DiureticDokumen3 halamanClassification of DiureticJanice Malafu De GuiaBelum ada peringkat
- DiureticsDokumen10 halamanDiureticsAyla NacariøBelum ada peringkat
- PHM - Hematologic DrugsDokumen3 halamanPHM - Hematologic DrugsJeanne Rodiño100% (3)
- Antihypertensive DrugsDokumen2 halamanAntihypertensive DrugsJillary LlagunoBelum ada peringkat
- Antiemetic Drugs PDFDokumen12 halamanAntiemetic Drugs PDFDanisha Laila100% (2)
- A.1. Community-Acquired: Use Antibiotics JudiciouslyDokumen33 halamanA.1. Community-Acquired: Use Antibiotics JudiciouslymaxgroovesBelum ada peringkat
- Anti-Arrhythmic Agents For Pharmacy PDFDokumen41 halamanAnti-Arrhythmic Agents For Pharmacy PDFKelvinTMaikanaBelum ada peringkat
- Diabetes Mellitus Drug ChartDokumen3 halamanDiabetes Mellitus Drug Chartlui.stephanie1751100% (1)
- Cholinergics and Cholinergic BlockersDokumen5 halamanCholinergics and Cholinergic Blockersapi-3739910100% (3)
- Gastrointestinal System and Nutrition Drug ChartsDokumen3 halamanGastrointestinal System and Nutrition Drug ChartsNursingSchoolNotesBelum ada peringkat
- AntiemeticsDokumen16 halamanAntiemeticswalt65Belum ada peringkat
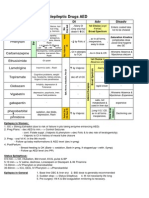
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDokumen1 halamanAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Belum ada peringkat
- Mu 002Dokumen10 halamanMu 002chandanBelum ada peringkat
- Antipsychotic Drugs: Conventional AntipsychoticsDokumen16 halamanAntipsychotic Drugs: Conventional AntipsychoticsApple MaeBelum ada peringkat
- Drug Cards EndoDokumen12 halamanDrug Cards EndoChristine Schroeder100% (1)
- Onco PharmacologyDokumen9 halamanOnco Pharmacologyarn0ld21Belum ada peringkat
- Major Pharm ReviewDokumen14 halamanMajor Pharm Reviewsarahpierre10100% (3)
- Antianginal DrugsDokumen3 halamanAntianginal DrugsyukariBelum ada peringkat
- Drugs WorksheetDokumen16 halamanDrugs Worksheetninja-2001Belum ada peringkat
- Agents Causing Coma or SeizuresDokumen3 halamanAgents Causing Coma or SeizuresShaira Aquino VerzosaBelum ada peringkat
- DiureticsDokumen75 halamanDiureticsSilpa Jayakumar100% (5)
- Cardiovascular DrugsDokumen6 halamanCardiovascular Drugslhayes123488% (16)
- Electrolyte Mnemonic QuizletDokumen3 halamanElectrolyte Mnemonic QuizletA.h.Murad100% (2)
- Endocrine Study GuideDokumen4 halamanEndocrine Study GuideNursingSchoolNotes100% (1)
- Anticoagulants DrugsDokumen6 halamanAnticoagulants DrugsHusam Al-OdatBelum ada peringkat
- Endocrine DisordersDokumen3 halamanEndocrine DisordersIrish OrleansBelum ada peringkat
- N196 GI Exam Study GuideDokumen7 halamanN196 GI Exam Study Guideaznknight3230% (1)
- Nursing Pharmacology Perfusion Study GuideDokumen9 halamanNursing Pharmacology Perfusion Study GuideChelsea SmithBelum ada peringkat
- Pharmacology SummaryDokumen16 halamanPharmacology Summaryshenric16Belum ada peringkat
- Anti Infective Drug ChartDokumen1 halamanAnti Infective Drug ChartJessica100% (1)
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideDari EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideBelum ada peringkat
- Ninja - Anemias PDFDokumen1 halamanNinja - Anemias PDFErica Hyeyeon LeeBelum ada peringkat
- Drug ChartDokumen20 halamanDrug Chartstarobin100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)Dari EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Belum ada peringkat
- Wps Gtaw Monel b127 b164Dokumen2 halamanWps Gtaw Monel b127 b164Srinivasan Muruganantham67% (3)
- Cad, CamDokumen16 halamanCad, CamRakhi Mol BVBelum ada peringkat
- Academic Program Required Recommended Academic Program Required RecommendedDokumen1 halamanAcademic Program Required Recommended Academic Program Required Recommendedonur scribdBelum ada peringkat
- Parts PrecedentDokumen252 halamanParts PrecedentOscar PinzonBelum ada peringkat
- Free-Field Equivalent Localization of Virtual AudioDokumen9 halamanFree-Field Equivalent Localization of Virtual AudiojulianpalacinoBelum ada peringkat
- 08 A330 Ata 35Dokumen32 halaman08 A330 Ata 35Owen100% (1)
- 34 Plaza Newsletter 101317 FINALDokumen4 halaman34 Plaza Newsletter 101317 FINALJosef SzendeBelum ada peringkat
- DysphagiaDokumen4 halamanDysphagiaMicaBelum ada peringkat
- Time Series - Practical ExercisesDokumen9 halamanTime Series - Practical ExercisesJobayer Islam TunanBelum ada peringkat
- Fill in The Table by Determining The Functions of The Following ItemsDokumen6 halamanFill in The Table by Determining The Functions of The Following ItemsJessabel CandidatoBelum ada peringkat
- Maximum Influence at A Point Dueto A Series of Concentrated LoadsDokumen12 halamanMaximum Influence at A Point Dueto A Series of Concentrated LoadsAyad SlabyBelum ada peringkat
- MPI Report 009 Sub Structure B668Dokumen1 halamanMPI Report 009 Sub Structure B668John DolanBelum ada peringkat
- Portable Manual - DIG-360Dokumen44 halamanPortable Manual - DIG-360waelmansour25Belum ada peringkat
- Parker Valve Safety CrownDokumen11 halamanParker Valve Safety Crownayman akrabBelum ada peringkat
- Biology Unit 4Dokumen44 halamanBiology Unit 4Mohammad KhanBelum ada peringkat
- Gmail - Welcome To Clarion Crossing!Dokumen4 halamanGmail - Welcome To Clarion Crossing!sagarnr gowdaBelum ada peringkat
- Pahlavi PoemDokumen9 halamanPahlavi PoemBatsuren BarangasBelum ada peringkat
- 2.PsychoCrash Social Psy-1Dokumen62 halaman2.PsychoCrash Social Psy-1Gopika Sureshnv0% (1)
- Anatomia Dezvoltarii PancreasuluiDokumen49 halamanAnatomia Dezvoltarii Pancreasuluitarra abuBelum ada peringkat
- Seminar1final ReviewDokumen19 halamanSeminar1final ReviewMounika ChBelum ada peringkat
- Short Moritz - LiverGB PDFDokumen3 halamanShort Moritz - LiverGB PDFPetra JobovaBelum ada peringkat
- Brief List of Temples in Haridwar Is Given BelowDokumen8 halamanBrief List of Temples in Haridwar Is Given BelowPritesh BamaniaBelum ada peringkat
- 1.toyotamarklogo Standard Jan 2021 eDokumen43 halaman1.toyotamarklogo Standard Jan 2021 eMercadeo TosakaBelum ada peringkat
- Fast Track Pro Drivers Read MeDokumen3 halamanFast Track Pro Drivers Read MeMatt JerniganBelum ada peringkat
- Pigging Training Course Mod 7 Rev 1Dokumen26 halamanPigging Training Course Mod 7 Rev 1Suparerk Sirivedin100% (1)
- Aipl2009 V120000001Dokumen7 halamanAipl2009 V120000001Olof HedinBelum ada peringkat
- Consent For Diagnostic And/or Therapeutic ParacentesisDokumen2 halamanConsent For Diagnostic And/or Therapeutic ParacentesisnaveenBelum ada peringkat
- Stahl - PUDSDokumen29 halamanStahl - PUDSsusanasusana_Belum ada peringkat
- X Glo LED Strip Lighting For Tunnelling BrochureDokumen6 halamanX Glo LED Strip Lighting For Tunnelling BrochureJOSE HUAMANIBelum ada peringkat