Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- UveitisDokumen10 halamanUveitisUtomo FemtomBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Contemporary Clinical Trials: Natalia A. Ricci, Mayra C. Aratani, Heloísa H. Caovilla, Fernando F. GanançaDokumen9 halamanContemporary Clinical Trials: Natalia A. Ricci, Mayra C. Aratani, Heloísa H. Caovilla, Fernando F. GanançaUtomo FemtomBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Tetanus: Pembimbing: Dr. Subandi, SP.S (K), FINACSDokumen27 halamanTetanus: Pembimbing: Dr. Subandi, SP.S (K), FINACSUtomo FemtomBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- FentanylDokumen12 halamanFentanylUtomo FemtomBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Jurnal InsomiaDokumen20 halamanJurnal InsomiaUtomo FemtomBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Insomnia 6Dokumen14 halamanInsomnia 6Utomo FemtomBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- IBH Link UA Manual PDFDokumen302 halamanIBH Link UA Manual PDFjavixl1Belum ada peringkat
- Häggloader 10HR-B: Atlas CopcoDokumen2 halamanHäggloader 10HR-B: Atlas CopcoHayam BaşaranBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Telmisartan, ISMNDokumen8 halamanTelmisartan, ISMNDenise EspinosaBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Forest Flower October 2018Dokumen24 halamanForest Flower October 2018RAGUNATH PBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Material Control Procedure - TemplateDokumen5 halamanMaterial Control Procedure - TemplateHernandito Rahmat KusumaBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- D20 25 30 33S-5 D35C-5 (Sb1109e06) PDFDokumen424 halamanD20 25 30 33S-5 D35C-5 (Sb1109e06) PDFGORD100% (8)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Maths Class Xii Sample Paper Test 02 For Board Exam 2023Dokumen6 halamanMaths Class Xii Sample Paper Test 02 For Board Exam 2023Priyanshu KasanaBelum ada peringkat
- MultiCrystallineDataSheet - EN - SilikenDokumen4 halamanMultiCrystallineDataSheet - EN - Silikensydneyaus2005Belum ada peringkat
- F115a'12 Fl115a'12: (68VB) (68WB)Dokumen96 halamanF115a'12 Fl115a'12: (68VB) (68WB)AlexDiazBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- SV9000 Series Products Intrduction PDFDokumen90 halamanSV9000 Series Products Intrduction PDFhamph113Belum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- DalmatiaDokumen265 halamanDalmatiaomissam2Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- SC607 Assignment2Dokumen2 halamanSC607 Assignment2Tirthankar AdhikariBelum ada peringkat
- Questions and Answers About Lead in Ceramic Tableware: Contra Costa Health Services / Lead Poisoning Prevention ProjectDokumen4 halamanQuestions and Answers About Lead in Ceramic Tableware: Contra Costa Health Services / Lead Poisoning Prevention Projectzorro21072107Belum ada peringkat
- Yamaha MG16 PDFDokumen2 halamanYamaha MG16 PDFmiskoyu027Belum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Portland PortDokumen18 halamanPortland PortAnonymous Lx3jPjHAVLBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Asms 02 0033Dokumen6 halamanAsms 02 0033Delfia AkiharyBelum ada peringkat
- Zen Intro To Buddhism & Practice of ZazenDokumen33 halamanZen Intro To Buddhism & Practice of ZazendudcomeonBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Unit-4 - Hypothesis TestingDokumen24 halamanUnit-4 - Hypothesis TestingMANTHAN JADHAVBelum ada peringkat
- Grade 7 Information Writing: The Bulldog: A Dog Like No OtherDokumen5 halamanGrade 7 Information Writing: The Bulldog: A Dog Like No Otherapi-202727113Belum ada peringkat
- Cengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test BankDokumen26 halamanCengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test Bankladonnaaidanm5s100% (28)
- Relay Identification: Example CDG31FF002SACHDokumen5 halamanRelay Identification: Example CDG31FF002SACHRohit RanaBelum ada peringkat
- Heil 4000 FeaturesDokumen1 halamanHeil 4000 FeaturesBogdan NgrBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Harrington SOAP NoteDokumen5 halamanHarrington SOAP NoteDanielle100% (4)
- Lesson Plan 1 - Agriculture in Your LifeDokumen6 halamanLesson Plan 1 - Agriculture in Your Lifeapi-235918896Belum ada peringkat
- Manuel D'utilisation Maison AnglaisDokumen17 halamanManuel D'utilisation Maison AnglaisVanesssBelum ada peringkat
- QW PDFDokumen45 halamanQW PDFkarthikeyan PBelum ada peringkat
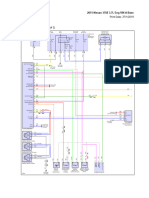
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDokumen69 halaman2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaBelum ada peringkat
- Lesson 4Dokumen10 halamanLesson 4Nagiri MuraliBelum ada peringkat
- Layout - Foundation Drawing - Air BlowerDokumen2 halamanLayout - Foundation Drawing - Air BlowerBabel THIAMBelum ada peringkat
- Nervous SystemDokumen40 halamanNervous SystemJaneBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)