Anda mungkin juga menyukai
- Disertasi Dr. TerawanDokumen8 halamanDisertasi Dr. TerawanNurhaidah AchmadBelum ada peringkat
- KADDokumen30 halamanKADDellBelum ada peringkat
- B135 Work and EpilepsyDokumen33 halamanB135 Work and EpilepsyDrSajid BuzdarBelum ada peringkat
- Nature CardiologyDokumen7 halamanNature CardiologyDellBelum ada peringkat
- KADDokumen30 halamanKADDellBelum ada peringkat
- Labour and Delivery Care Module - 4 Using The Partograph - View As Single PageDokumen21 halamanLabour and Delivery Care Module - 4 Using The Partograph - View As Single PageDellBelum ada peringkat
- Module 14 Pediatric TB ENGLISHDokumen85 halamanModule 14 Pediatric TB ENGLISHDellBelum ada peringkat
- Sliwa Et Al-2017-European Journal of Heart FailureDokumen11 halamanSliwa Et Al-2017-European Journal of Heart FailureDellBelum ada peringkat
- Sliwa Et Al-2017-European Journal of Heart FailureDokumen11 halamanSliwa Et Al-2017-European Journal of Heart FailureDellBelum ada peringkat
- GLM0021 Postpartum HaemorrhageDokumen13 halamanGLM0021 Postpartum HaemorrhageDellBelum ada peringkat
- SalerioDokumen28 halamanSalerioRizqaFebrilianyBelum ada peringkat
- Clinical Yeoh PDFDokumen5 halamanClinical Yeoh PDFAzizan HannyBelum ada peringkat
- Year 4 OSCEguideDokumen159 halamanYear 4 OSCEguideDrSajid BuzdarBelum ada peringkat
- Year 4 OSCEguideDokumen159 halamanYear 4 OSCEguideDrSajid BuzdarBelum ada peringkat
- HTN Late PregnancyDokumen2 halamanHTN Late PregnancyDellBelum ada peringkat
- 5 Morisky Medication Adherence-Scale PDFDokumen1 halaman5 Morisky Medication Adherence-Scale PDFDellBelum ada peringkat
- Clinical Diagnosis and Complications of Paratubal Cysts: Review of The Literature and Report of Uncommon PresentationsDokumen10 halamanClinical Diagnosis and Complications of Paratubal Cysts: Review of The Literature and Report of Uncommon PresentationsDellBelum ada peringkat
- Family Planning HandbookDokumen387 halamanFamily Planning HandbookvthiseasBelum ada peringkat
- Fitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDokumen30 halamanFitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDellBelum ada peringkat
- Jurnal Farmakologi Anti Konvulsi PDFDokumen13 halamanJurnal Farmakologi Anti Konvulsi PDFtherempongss100% (1)
- SPSS Crosstab PDFDokumen3 halamanSPSS Crosstab PDFDellBelum ada peringkat
- A Practical Classification of Septonasal Deviation.42Dokumen3 halamanA Practical Classification of Septonasal Deviation.42DellBelum ada peringkat
- Journal Pone 0158499Dokumen11 halamanJournal Pone 0158499DellBelum ada peringkat
- NICEguidelineonAEDsAugust2014 0Dokumen3 halamanNICEguidelineonAEDsAugust2014 0DellBelum ada peringkat
- CE-Hypertension The Silent KillerDokumen8 halamanCE-Hypertension The Silent KillerD.E.P.HBelum ada peringkat
- CTG Classification PDFDokumen1 halamanCTG Classification PDFDellBelum ada peringkat
- TB CutisDokumen16 halamanTB CutisDellBelum ada peringkat
- 144TD (C) 25 (E3) - Issue No 3 - Ear, Nose and Throat (ENT) Infections Antibiotic Guidelines PDFDokumen9 halaman144TD (C) 25 (E3) - Issue No 3 - Ear, Nose and Throat (ENT) Infections Antibiotic Guidelines PDFDellBelum ada peringkat
- Jnma00266 0071Dokumen4 halamanJnma00266 0071DellBelum ada peringkat
- Functional Endoscopic Sinus Surgery - American Family PhysicianDokumen8 halamanFunctional Endoscopic Sinus Surgery - American Family PhysicianDellBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Raynaud Phenomenon Practice Essentials: View Media Gallery Cutaneous Clues To Accurately Diagnosing Rheumatologic DiseaseDokumen2 halamanRaynaud Phenomenon Practice Essentials: View Media Gallery Cutaneous Clues To Accurately Diagnosing Rheumatologic DiseasedhiyarahadianBelum ada peringkat
- Ozone Therapy Conference at Bombay Hospital Focuses On Shared ExperiencesDokumen4 halamanOzone Therapy Conference at Bombay Hospital Focuses On Shared ExperiencesDr Saxena Centre for Progressive MedicineBelum ada peringkat
- Medstar Obgyn 1st EditionDokumen320 halamanMedstar Obgyn 1st Editionfetene82% (11)
- The Periodic Health ExaminationDokumen30 halamanThe Periodic Health ExaminationabstabsBelum ada peringkat
- Advanced Practice Nursing PhilosophyDokumen10 halamanAdvanced Practice Nursing Philosophyfmiller001Belum ada peringkat
- Teen 2 Teen Entire Curriculum Guide For PresentersDokumen113 halamanTeen 2 Teen Entire Curriculum Guide For PresentersElena Rusu50% (2)
- Uncovering the mystery behind the coronavirus pandemicDokumen7 halamanUncovering the mystery behind the coronavirus pandemickim VERGARABelum ada peringkat
- Mental health and HIV in IndiaDokumen7 halamanMental health and HIV in IndiaAyu RajikanBelum ada peringkat
- Preceptor Evaluation of Hannah LaiDokumen2 halamanPreceptor Evaluation of Hannah Laiapi-417446716Belum ada peringkat
- Tabel Penetapan Prioritas 5 ILMDokumen12 halamanTabel Penetapan Prioritas 5 ILMyantiBelum ada peringkat
- Prof Chris Chan Yin WeiDokumen6 halamanProf Chris Chan Yin WeiDavid PalashBelum ada peringkat
- Deafness & Hearing LossDokumen39 halamanDeafness & Hearing LossjialeongBelum ada peringkat
- A Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFDokumen7 halamanA Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFHemin HassanBelum ada peringkat
- Dermatology Secrets Plus 4th Edition ReviewDokumen1 halamanDermatology Secrets Plus 4th Edition ReviewYoga Adi0% (2)
- M. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingDokumen11 halamanM. Sc. Nursing Programme Analysis: Post-Graduate Education-Msc NursingMallika JoonBelum ada peringkat
- Rapid Disability Rating ScaleDokumen3 halamanRapid Disability Rating ScaleFatmawatiBelum ada peringkat
- Overweight 2Dokumen1 halamanOverweight 2Trần NhânBelum ada peringkat
- Adverse Drug ReactionsDokumen21 halamanAdverse Drug ReactionsRohit100% (1)
- Guidelines For Toxicity/safety Profile Evaluation of Ayurved & Siddha, Plant DrugsDokumen5 halamanGuidelines For Toxicity/safety Profile Evaluation of Ayurved & Siddha, Plant DrugsPRAKASH DESHPANDEBelum ada peringkat
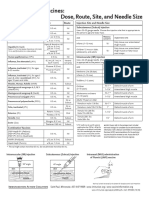
- Injection Site and Needle Size Vaccine Dose RouteDokumen1 halamanInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaBelum ada peringkat
- Preterm Labor and PROMDokumen102 halamanPreterm Labor and PROMDan Matthew BuriasBelum ada peringkat
- Chapter 24: Injury Prevention and Child Maltreatment Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDokumen2 halamanChapter 24: Injury Prevention and Child Maltreatment Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuBelum ada peringkat
- Torch InfectionsDokumen13 halamanTorch InfectionsOmeBelum ada peringkat
- VaticanDokumen6 halamanVaticanLucia AndreeaBelum ada peringkat
- NCP DRDokumen3 halamanNCP DRRhuwelyn Parantar PilapilBelum ada peringkat
- Thyroid Disorders Part II Hypothyroidism and Thyroiditis LIttle 2006Dokumen6 halamanThyroid Disorders Part II Hypothyroidism and Thyroiditis LIttle 2006Jing XueBelum ada peringkat
- Drug Proving Project InvestigationsDokumen8 halamanDrug Proving Project InvestigationsJayBelum ada peringkat
- Arabic WordsDokumen17 halamanArabic WordsWEBSTER LOPEZBelum ada peringkat
- Useful Vocabs For OET Writing & Speaking PDFDokumen2 halamanUseful Vocabs For OET Writing & Speaking PDFLiju K Oommen100% (3)
- Nanoparticles in Drug Loading Encapsulation and Adsorption-2019-03-31-20-59 PDFDokumen3 halamanNanoparticles in Drug Loading Encapsulation and Adsorption-2019-03-31-20-59 PDFsara castro olayaBelum ada peringkat