Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Module 14 Pediatric TB ENGLISHDokumen85 halamanModule 14 Pediatric TB ENGLISHDellBelum ada peringkat
- 5 Morisky Medication Adherence-Scale PDFDokumen1 halaman5 Morisky Medication Adherence-Scale PDFDellBelum ada peringkat
- Family Planning HandbookDokumen387 halamanFamily Planning HandbookvthiseasBelum ada peringkat
- Jurnal Farmakologi Anti Konvulsi PDFDokumen13 halamanJurnal Farmakologi Anti Konvulsi PDFtherempongss100% (1)
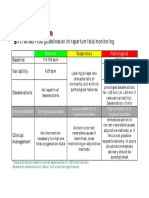
- CTG Classification PDFDokumen1 halamanCTG Classification PDFDellBelum ada peringkat
- 5 Morisky Medication Adherence-Scale PDFDokumen1 halaman5 Morisky Medication Adherence-Scale PDFDellBelum ada peringkat
- SPSS Crosstab PDFDokumen3 halamanSPSS Crosstab PDFDellBelum ada peringkat
- A Practical Classification of Septonasal Deviation.42Dokumen3 halamanA Practical Classification of Septonasal Deviation.42DellBelum ada peringkat
- Fitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDokumen30 halamanFitzpatrick's Dermatology in General Medicine, Eighth Edition, 2 Volume SetDellBelum ada peringkat
- Appendix 8 Normal Urine Output PDFDokumen1 halamanAppendix 8 Normal Urine Output PDFDellBelum ada peringkat
- Cutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDokumen10 halamanCutaneous Tuberculosis: Epidemiologic, Etiopathogenic and Clinical Aspects - Part IDellBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- English10 Q3 LC3Dokumen12 halamanEnglish10 Q3 LC3Ivy SalazarBelum ada peringkat
- Copy (2) of ThesisDokumen20 halamanCopy (2) of Thesiscaridadlintao100% (1)
- Quarter 1 Perform Hand SpaDokumen10 halamanQuarter 1 Perform Hand SpaDrexler LabagalaBelum ada peringkat
- Patrick BBDokumen8 halamanPatrick BBTiffany Sabilla RamadhaniBelum ada peringkat
- (Pha6114 Lec) 1ST Shifting ReviewerDokumen88 halaman(Pha6114 Lec) 1ST Shifting ReviewerAndrei RoqueBelum ada peringkat
- Avian Influenza in ChickensDokumen19 halamanAvian Influenza in ChickensShah NawazBelum ada peringkat
- 150 Question Labce Quez. 1 PDFDokumen87 halaman150 Question Labce Quez. 1 PDFadvance ascpBelum ada peringkat
- 8 L 1 1-Viruses Bacteria Fungi and ParasitesDokumen61 halaman8 L 1 1-Viruses Bacteria Fungi and Parasitesapi-290100812Belum ada peringkat
- Malubay RW01Dokumen5 halamanMalubay RW01ria ricciBelum ada peringkat
- Iso 22442-1-2015Dokumen34 halamanIso 22442-1-2015iipmnpti iipmBelum ada peringkat
- Park SoftDokumen942 halamanPark Softnaresh chauhanBelum ada peringkat
- Dr. Dian Nurul Al Amini, SP - THTDokumen6 halamanDr. Dian Nurul Al Amini, SP - THTRifaniNugrohoBelum ada peringkat
- What Are Koch's Postulates?Dokumen3 halamanWhat Are Koch's Postulates?Cacamo Rexell-anBelum ada peringkat
- K.N.ravichitra, Et AlDokumen5 halamanK.N.ravichitra, Et AldindaBelum ada peringkat
- Mylonakis Et Al. 2019Dokumen9 halamanMylonakis Et Al. 2019pablocrodriguezBelum ada peringkat
- FamcomDokumen2 halamanFamcomFeyre LunaBelum ada peringkat
- Corona Virus Tanishq PPT Project (Autosaved)Dokumen30 halamanCorona Virus Tanishq PPT Project (Autosaved)tanishq dafaleBelum ada peringkat
- Personal HygieneDokumen6 halamanPersonal HygieneRespicio Christian Aejay G.Belum ada peringkat
- Microbiology 2Dokumen53 halamanMicrobiology 2pikachuBelum ada peringkat
- Chronicles of Darkness The Contagion ChronicleDokumen287 halamanChronicles of Darkness The Contagion ChronicleBruno Estevão Gonzaga Dias100% (9)
- MEASLES and MALARIADokumen19 halamanMEASLES and MALARIADoreen Claire M. WallangBelum ada peringkat
- M10 FundaDokumen6 halamanM10 FundaAl-Khan HadjailBelum ada peringkat
- Predictors of Intention To Vaccinate Against COVID-19: Results of A Nationwide SurveyDokumen7 halamanPredictors of Intention To Vaccinate Against COVID-19: Results of A Nationwide SurveyDika MidbrainBelum ada peringkat
- EVE Online Chronicles PDFDokumen1.644 halamanEVE Online Chronicles PDFRazvan Emanuel GheorgheBelum ada peringkat
- New Classification and Colour Code Development For An Efficient Medical Waste SegregationDokumen12 halamanNew Classification and Colour Code Development For An Efficient Medical Waste SegregationGlobal Research and Development ServicesBelum ada peringkat
- Product Preview 2Dokumen20 halamanProduct Preview 2Dong Zhang100% (1)
- Topic 24 Health Diagnosis, Prevention, and HealingDokumen3 halamanTopic 24 Health Diagnosis, Prevention, and HealingMarilyn DizonBelum ada peringkat
- 1996 A I A GuidelinesDokumen12 halaman1996 A I A Guidelinesoli san miguelBelum ada peringkat
- Unefm - Uptjr: Bolivarian Republic of Venezuela Ministry of Popular Power For Higher EducationDokumen8 halamanUnefm - Uptjr: Bolivarian Republic of Venezuela Ministry of Popular Power For Higher EducationRonald BohadaBelum ada peringkat
- The Evolution and Importance of Vaccines in Public HealthDokumen2 halamanThe Evolution and Importance of Vaccines in Public HealthHiroBelum ada peringkat