Anda mungkin juga menyukai
- 11 Topnotch Pediatrics SuperExam PDFDokumen97 halaman11 Topnotch Pediatrics SuperExam PDFDre Valdez100% (4)
- S5-42 DatasheetDokumen2 halamanS5-42 Datasheetchillin_in_bots100% (1)
- Two Mechanisms of Hypertensive NephrosclerosisDokumen2 halamanTwo Mechanisms of Hypertensive NephrosclerosisJessica Damasen Caballero0% (1)
- Pathophysiology of ESRD: Organ Dysfunctions & Associated AbnormalitiesDokumen5 halamanPathophysiology of ESRD: Organ Dysfunctions & Associated AbnormalitiesCarl JardelezaBelum ada peringkat
- Left-Sided Heart FailureDokumen3 halamanLeft-Sided Heart FailureKhalid Mahmud ArifinBelum ada peringkat
- Pill-Popping Gone Bad - The Antibiotic Self-Medication Practices of Residents of Iloilo CityDokumen18 halamanPill-Popping Gone Bad - The Antibiotic Self-Medication Practices of Residents of Iloilo CityBryan LadridoBelum ada peringkat
- HCVDDokumen5 halamanHCVDkhrizaleehBelum ada peringkat
- Hypertensive NephrosclerosisDokumen14 halamanHypertensive Nephrosclerosisreysanne100% (1)
- Understanding Stevens-Johnson Syndrome (SJSDokumen53 halamanUnderstanding Stevens-Johnson Syndrome (SJSKathrina CraveBelum ada peringkat
- Patho Pleural EffusionDokumen2 halamanPatho Pleural EffusionJess Prodigo50% (2)
- Hypertension: Colegio de San Juan de LetranDokumen13 halamanHypertension: Colegio de San Juan de LetranJenna AbuanBelum ada peringkat
- Gallstones Case StudyDokumen70 halamanGallstones Case StudyIrize DenagaBelum ada peringkat
- ThiazideDokumen4 halamanThiazideEkarthi KeyanBelum ada peringkat
- NPI Feb2,7 And8Dokumen14 halamanNPI Feb2,7 And8Mikko Anthony Pingol AlarconBelum ada peringkat
- Hypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood PressureDokumen3 halamanHypertensive Cardiovascular Disease Also Known As Hypertensive Heart Disease Occurs Due To The Complication of Hypertension or High Blood Pressurejoanneceline16Belum ada peringkat
- PATHOPHYSIOLOGY PancreatitisDokumen1 halamanPATHOPHYSIOLOGY PancreatitisMicahEuranneCastillo-GoliBelum ada peringkat
- Concept Map of CKD Gastrointestinal SymptomsDokumen4 halamanConcept Map of CKD Gastrointestinal SymptomsWendy Escalante0% (1)
- Electrolyte Imbalance NCPDokumen6 halamanElectrolyte Imbalance NCPjohnart jimenezBelum ada peringkat
- CVA PathophysiologyDokumen3 halamanCVA Pathophysiologyshmily_0810Belum ada peringkat
- Pathophysiology of Diabetes Mellitus Type II and NephrolithiasisDokumen6 halamanPathophysiology of Diabetes Mellitus Type II and Nephrolithiasisdiane_mananganBelum ada peringkat
- Reflection PaperDokumen2 halamanReflection PapershanoiapowelllBelum ada peringkat
- CHRONIC HEART FAILURE CASE STUDYDokumen12 halamanCHRONIC HEART FAILURE CASE STUDYMary Cris CanonBelum ada peringkat
- Nursing Care Plan For Myocardial InfarctionDokumen1 halamanNursing Care Plan For Myocardial InfarctionIshaBrijeshSharmaBelum ada peringkat
- Pathophysiology HPN CvaDokumen1 halamanPathophysiology HPN Cvatresdos09Belum ada peringkat
- Hypertensive Cardiovascular DiseaseDokumen5 halamanHypertensive Cardiovascular DiseaseAna Katrina OcanaBelum ada peringkat
- Neurogenic ShockDokumen3 halamanNeurogenic ShockGlaizalyn Fabella TagoonBelum ada peringkat
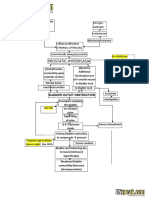
- Benign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFDokumen2 halamanBenign Prostatic Hyperplasia BPH Pathophysiology Schematic Diagram PDFgailBelum ada peringkat
- Pathophysiology Diagram of Congestive Heart FailureDokumen3 halamanPathophysiology Diagram of Congestive Heart FailureLeng Royo BrionesBelum ada peringkat
- PathophysiologyDokumen9 halamanPathophysiologySuzette PipoBelum ada peringkat
- Multiple Physical Injuries Secondary To Vehicular AccidentDokumen31 halamanMultiple Physical Injuries Secondary To Vehicular AccidentJane Arian BerzabalBelum ada peringkat
- ASSESSMENT EXPLANATION OF THE OBJECTIVES NURSING INTERVENTIONS RATIONALE EVALUATIONDokumen5 halamanASSESSMENT EXPLANATION OF THE OBJECTIVES NURSING INTERVENTIONS RATIONALE EVALUATIONRussel SantosBelum ada peringkat
- Path o PhysiologyDokumen9 halamanPath o PhysiologyKyle Ü D. CunanersBelum ada peringkat
- Congestive Heart FailureDokumen4 halamanCongestive Heart FailureAnnie Grace PoliranBelum ada peringkat
- Nephrolithiasis PDFDokumen16 halamanNephrolithiasis PDFApriany Cordias Arlita SilalahiBelum ada peringkat
- Impaired Tissue PerfusionDokumen2 halamanImpaired Tissue PerfusionLyka Mae Imbat - PacnisBelum ada peringkat
- MI Case Study FinalDokumen25 halamanMI Case Study FinalAlmaBelum ada peringkat
- Pathophysiology of Patent Ductus Arteroisus (PDA)Dokumen2 halamanPathophysiology of Patent Ductus Arteroisus (PDA)Rodel YacasBelum ada peringkat
- CKD - For Concept MappingDokumen7 halamanCKD - For Concept MappingKennette Lim0% (1)
- Assessment Nursing Diagnosis Planning Nursing Intervention Rationale EvaluationDokumen3 halamanAssessment Nursing Diagnosis Planning Nursing Intervention Rationale EvaluationMikhaelEarlSantosTacordaBelum ada peringkat
- Hypertension Obstruction: Chronic Renal FailureDokumen3 halamanHypertension Obstruction: Chronic Renal FailureDiane-Richie PezLo100% (1)
- Risk For Bleeding - Cirrhosis NCPDokumen2 halamanRisk For Bleeding - Cirrhosis NCPPaula AbadBelum ada peringkat
- Learning Zone: Chronic Kidney Disease: Risk Factors, Assessment and Nursing CareDokumen8 halamanLearning Zone: Chronic Kidney Disease: Risk Factors, Assessment and Nursing CareDennis CobbBelum ada peringkat
- Discharge PlanDokumen1 halamanDischarge PlanLeolene Grace BautistaBelum ada peringkat
- Osteoarthritis 1583-170210113823Dokumen34 halamanOsteoarthritis 1583-170210113823Angelic khanBelum ada peringkat
- Age Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat IntakeDokumen3 halamanAge Greater Than 60 Y/o Hereditary Precipitating Factors: Hypertension Increase Protein and Fat Intakenursing concept mapsBelum ada peringkat
- PyomyositisDokumen31 halamanPyomyositisAezl Mercado0% (1)
- Patient Education: A Guide for NursesDokumen32 halamanPatient Education: A Guide for Nursesاسامة محمد السيد رمضانBelum ada peringkat
- SLE Risk Factors and ComplicationsDokumen5 halamanSLE Risk Factors and Complicationsjoyrena ochondraBelum ada peringkat
- Pathophysiology of AtherosclerosisDokumen1 halamanPathophysiology of AtherosclerosisAzrul Hakim100% (2)
- NCM 103 (RLE) : Bangued, AbraDokumen26 halamanNCM 103 (RLE) : Bangued, AbraMhalynne Eduarte- BayonganBelum ada peringkat
- Drug StudyDokumen8 halamanDrug StudyJohn Ronald P. RamosBelum ada peringkat
- Benign Prostatic Hyperplasia (BPH) PDFDokumen5 halamanBenign Prostatic Hyperplasia (BPH) PDFKhuswatun Hasanah100% (1)
- ACS SchematicDokumen2 halamanACS Schematicswish27Belum ada peringkat
- Case Study-Acute Urinary RetentionDokumen10 halamanCase Study-Acute Urinary RetentionArthadian De Peralta75% (4)
- Pathophysiology of Heart Failure Due to Myocardial DysfunctionDokumen1 halamanPathophysiology of Heart Failure Due to Myocardial DysfunctionabbeeyyBelum ada peringkat
- Pathophysiology CVD InfarctDokumen1 halamanPathophysiology CVD InfarctElisa KerrBelum ada peringkat
- NCP Ineffective Cardiopulmonary PerfusionDokumen3 halamanNCP Ineffective Cardiopulmonary PerfusionjamiemapanaoBelum ada peringkat
- Queenie Rose Domingo - Drug Study (Silver Sulfadiazine)Dokumen1 halamanQueenie Rose Domingo - Drug Study (Silver Sulfadiazine)Sheryl Ann Barit PedinesBelum ada peringkat
- Hirschprungs DiseaseDokumen26 halamanHirschprungs DiseaseAndrian PramanaBelum ada peringkat
- Renal Vascular Disease GuideDokumen46 halamanRenal Vascular Disease GuideCoy NuñezBelum ada peringkat
- Hypertension Management in Diabetes: Blood Pressure Targets and TreatmentDokumen6 halamanHypertension Management in Diabetes: Blood Pressure Targets and TreatmentNorma González CervantesBelum ada peringkat
- Stages of Chronic Kidney Disease Stage Description GFR Ml/min/1.73mDokumen4 halamanStages of Chronic Kidney Disease Stage Description GFR Ml/min/1.73mMegan SamsonBelum ada peringkat
- FAM MED COVID 19 by SC Rana RojoDokumen112 halamanFAM MED COVID 19 by SC Rana RojoAllene PaderangaBelum ada peringkat
- Drug InfographicsDokumen8 halamanDrug InfographicsAllene PaderangaBelum ada peringkat
- IV Antibiotics Dosing and Preparation GuideDokumen2 halamanIV Antibiotics Dosing and Preparation GuideAllene PaderangaBelum ada peringkat
- Pedia Case ProtocolDokumen5 halamanPedia Case ProtocolAllene PaderangaBelum ada peringkat
- CestodesDokumen3 halamanCestodesAllene PaderangaBelum ada peringkat
- 2.27 (FCM) Strategies For COVID-19Dokumen9 halaman2.27 (FCM) Strategies For COVID-19Allene PaderangaBelum ada peringkat
- 1.07 (OB-CK) Second Stage of LaborDokumen9 halaman1.07 (OB-CK) Second Stage of LaborAllene PaderangaBelum ada peringkat
- Xavier University Medical Student Attitude EvaluationDokumen1 halamanXavier University Medical Student Attitude EvaluationAllene PaderangaBelum ada peringkat
- 1.63 Gyne Abnormal Uterine Bleeding 1Dokumen6 halaman1.63 Gyne Abnormal Uterine Bleeding 1Allene PaderangaBelum ada peringkat
- Breast SchwartzDokumen72 halamanBreast SchwartzAllene PaderangaBelum ada peringkat
- PDR HISTORY TAKING PEDIA HX ClinicsDokumen11 halamanPDR HISTORY TAKING PEDIA HX ClinicsAllene PaderangaBelum ada peringkat
- Body temperature, vital signs, anthropometric measurementsDokumen8 halamanBody temperature, vital signs, anthropometric measurementsApril Rae Obregon GarcesBelum ada peringkat
- 2.43 (FCM) Logic ModelsDokumen6 halaman2.43 (FCM) Logic ModelsAllene PaderangaBelum ada peringkat
- Anatomy of the EarDokumen12 halamanAnatomy of the EarAllene PaderangaBelum ada peringkat
- Introduction To Reconstructive and Aesthetic Plastic SurgeryDokumen15 halamanIntroduction To Reconstructive and Aesthetic Plastic SurgeryAllene PaderangaBelum ada peringkat
- Drug ScriptDokumen1 halamanDrug ScriptAllene PaderangaBelum ada peringkat
- PDR Respiratory System Thorax LungsDokumen4 halamanPDR Respiratory System Thorax LungsAllene PaderangaBelum ada peringkat
- French Toast Baked Omelette Breakfast Tacos Belgian Waffles Egg CasseroleDokumen7 halamanFrench Toast Baked Omelette Breakfast Tacos Belgian Waffles Egg CasseroleAllene PaderangaBelum ada peringkat
- The Galing Pook Awards Research ResultsDokumen5 halamanThe Galing Pook Awards Research ResultsAllene PaderangaBelum ada peringkat
- Trematode SDokumen2 halamanTrematode SAllene PaderangaBelum ada peringkat
- CestodesDokumen3 halamanCestodesAllene PaderangaBelum ada peringkat
- Drug ScriptDokumen1 halamanDrug ScriptAllene PaderangaBelum ada peringkat
- Shalai Catering ServicesDokumen4 halamanShalai Catering ServicesAllene PaderangaBelum ada peringkat
- 1Dokumen3 halaman1Allene PaderangaBelum ada peringkat
- Trematode SDokumen2 halamanTrematode SAllene PaderangaBelum ada peringkat
- Cerebrum, Ventricular SystemDokumen3 halamanCerebrum, Ventricular SystemAllene PaderangaBelum ada peringkat
- Female Repro HistoDokumen26 halamanFemale Repro HistoAllene PaderangaBelum ada peringkat
- Hypothalamic-Pituitary Endocrine Axis and Posterior Pituitary HormonesDokumen11 halamanHypothalamic-Pituitary Endocrine Axis and Posterior Pituitary HormonesAllene PaderangaBelum ada peringkat
- Transport of Sodium and ChlorideDokumen12 halamanTransport of Sodium and ChlorideAllene PaderangaBelum ada peringkat
- Level 3 Repair PBA Parts LayoutDokumen32 halamanLevel 3 Repair PBA Parts LayoutabivecueBelum ada peringkat
- Contact and Profile of Anam ShahidDokumen1 halamanContact and Profile of Anam ShahidSchengen Travel & TourismBelum ada peringkat
- KPMG Inpection ReportDokumen11 halamanKPMG Inpection ReportMacharia NgunjiriBelum ada peringkat
- Take This LoveDokumen2 halamanTake This LoveRicardo Saul LaRosaBelum ada peringkat
- Preventing and Mitigating COVID-19 at Work: Policy Brief 19 May 2021Dokumen21 halamanPreventing and Mitigating COVID-19 at Work: Policy Brief 19 May 2021Desy Fitriani SarahBelum ada peringkat
- CAS-GEC04 Module11 Food-SecurityDokumen6 halamanCAS-GEC04 Module11 Food-SecurityPermalino Borja Rose AnneBelum ada peringkat
- Borello-Bolted Steel Slip-Critical Connections With Fillers I. PerformanceDokumen10 halamanBorello-Bolted Steel Slip-Critical Connections With Fillers I. PerformanceaykutBelum ada peringkat
- Cold Rolled Steel Sections - Specification: Kenya StandardDokumen21 halamanCold Rolled Steel Sections - Specification: Kenya StandardPEng. Tech. Alvince KoreroBelum ada peringkat
- Tigo Pesa Account StatementDokumen7 halamanTigo Pesa Account StatementPeter Ngicur Carthemi100% (1)
- Pita Cyrel R. Activity 7Dokumen5 halamanPita Cyrel R. Activity 7Lucky Lynn AbreraBelum ada peringkat
- Motor Master 20000 SeriesDokumen56 halamanMotor Master 20000 SeriesArnulfo Lavares100% (1)
- Chennai Metro Rail BoQ for Tunnel WorksDokumen6 halamanChennai Metro Rail BoQ for Tunnel WorksDEBASIS BARMANBelum ada peringkat
- Nursing Care Management of a Client with Multiple Medical ConditionsDokumen25 halamanNursing Care Management of a Client with Multiple Medical ConditionsDeannBelum ada peringkat
- Difference Between Text and Discourse: The Agent FactorDokumen4 halamanDifference Between Text and Discourse: The Agent FactorBenjamin Paner100% (1)
- 50 Years of Teaching PianoDokumen122 halaman50 Years of Teaching PianoMyklan100% (35)
- How Psychology Has Changed Over TimeDokumen2 halamanHow Psychology Has Changed Over TimeMaedot HaddisBelum ada peringkat
- Wasserman Chest 1997Dokumen13 halamanWasserman Chest 1997Filip BreskvarBelum ada peringkat
- DNA Gel Electrophoresis Lab Solves MysteryDokumen8 halamanDNA Gel Electrophoresis Lab Solves MysteryAmit KumarBelum ada peringkat
- Rishte ki baat SMS messages collectionDokumen108 halamanRishte ki baat SMS messages collectionTushar AggarwalBelum ada peringkat
- Fernandez ArmestoDokumen10 halamanFernandez Armestosrodriguezlorenzo3288Belum ada peringkat
- Good Ethics Is Good BusinessDokumen9 halamanGood Ethics Is Good BusinesssumeetpatnaikBelum ada peringkat
- Evaluating MYP Rubrics in WORDDokumen11 halamanEvaluating MYP Rubrics in WORDJoseph VEGABelum ada peringkat
- Radio Frequency Transmitter Type 1: System OperationDokumen2 halamanRadio Frequency Transmitter Type 1: System OperationAnonymous qjoKrp0oBelum ada peringkat
- Resume Template & Cover Letter Bu YoDokumen4 halamanResume Template & Cover Letter Bu YoRifqi MuttaqinBelum ada peringkat
- 2023-Physics-Informed Radial Basis Network (PIRBN) A LocalDokumen41 halaman2023-Physics-Informed Radial Basis Network (PIRBN) A LocalmaycvcBelum ada peringkat
- 17BCE0552 Java DA1 PDFDokumen10 halaman17BCE0552 Java DA1 PDFABHIMAYU JENABelum ada peringkat
- AgentScope: A Flexible Yet Robust Multi-Agent PlatformDokumen24 halamanAgentScope: A Flexible Yet Robust Multi-Agent PlatformRijalBelum ada peringkat
- Kami Export - BuildingtheTranscontinentalRailroadWEBQUESTUsesQRCodes-1Dokumen3 halamanKami Export - BuildingtheTranscontinentalRailroadWEBQUESTUsesQRCodes-1Anna HattenBelum ada peringkat
- Axe Case Study - Call Me NowDokumen6 halamanAxe Case Study - Call Me NowvirgoashishBelum ada peringkat