Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- High Yield Internal Medicine Shelf Exam ReviewDokumen100 halamanHigh Yield Internal Medicine Shelf Exam ReviewAhsan X Baig100% (5)
- High Yield Surgery Shelf ReviewDokumen77 halamanHigh Yield Surgery Shelf ReviewDuke71% (7)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- OMT ReviewDokumen114 halamanOMT Reviewvin100% (2)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Surgical Notes A Pocket Survival GuideDokumen197 halamanSurgical Notes A Pocket Survival Guidevin100% (12)
- Einstein Quotes On SpiritualityDokumen2 halamanEinstein Quotes On Spiritualitybob jamesBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- TirukuralDokumen623 halamanTirukuralvin100% (2)
- STSDSD QuestionDokumen12 halamanSTSDSD QuestionAakash DasBelum ada peringkat
- Army National Guard Military Funeral Honors Soldier S Training SOP 23 Nov 15Dokumen203 halamanArmy National Guard Military Funeral Honors Soldier S Training SOP 23 Nov 15LuisAndresBellavista100% (1)
- Integrative Paper Unfolding The SelfDokumen11 halamanIntegrative Paper Unfolding The SelfTrentox XXXBelum ada peringkat
- Suntay V CojuancoDokumen2 halamanSuntay V CojuancoJushiBelum ada peringkat
- Geriatrics Article On NutritionDokumen10 halamanGeriatrics Article On NutritionvinBelum ada peringkat
- A.A AntagonismDokumen19 halamanA.A Antagonismjraj030_2k6Belum ada peringkat
- Importers in BOC List As of June 2, 2015Dokumen254 halamanImporters in BOC List As of June 2, 2015PortCalls88% (8)
- Cards/Tables 48 hrs before new lessonsDokumen1 halamanCards/Tables 48 hrs before new lessonsvinBelum ada peringkat
- Sample Step 1 ScheduleDokumen2 halamanSample Step 1 ScheduleAmparo Cortes IllanesBelum ada peringkat
- AnatomyDokumen4 halamanAnatomyvinBelum ada peringkat
- Type I HSDokumen3 halamanType I HSvinBelum ada peringkat
- Renal 1 - Anatomy, Em, HistoDokumen24 halamanRenal 1 - Anatomy, Em, HistovinBelum ada peringkat
- High Yield EmbryologyDokumen14 halamanHigh Yield EmbryologyvinBelum ada peringkat
- Renal ClinicalDokumen7 halamanRenal ClinicalvinBelum ada peringkat
- CardiologyDokumen32 halamanCardiologyvinBelum ada peringkat
- Hodgkins ChartsDokumen3 halamanHodgkins ChartsvinBelum ada peringkat
- Cardiac TransplantDokumen27 halamanCardiac TransplantvinBelum ada peringkat
- Feature Hepatitis A Hepatitis B Hepatitis C: Common Name Virus Structure Transmission Onset Incubation Period (Days)Dokumen2 halamanFeature Hepatitis A Hepatitis B Hepatitis C: Common Name Virus Structure Transmission Onset Incubation Period (Days)vinBelum ada peringkat
- Heart Sounds OutlineDokumen31 halamanHeart Sounds OutlinevinBelum ada peringkat
- Duties of Trustees ExplainedDokumen39 halamanDuties of Trustees ExplainedZia IzaziBelum ada peringkat
- A Project Report On Working Capital Management of Hindalco For The Last Five YearsDokumen83 halamanA Project Report On Working Capital Management of Hindalco For The Last Five YearsBabasab Patil (Karrisatte)0% (1)
- VET PREVENTIVE MEDICINE EXAMDokumen8 halamanVET PREVENTIVE MEDICINE EXAMashish kumarBelum ada peringkat
- An Equivalent SDOF System Model For Estimating The Earthquake Response of R/C Buildings With Hysteretic DampersDokumen8 halamanAn Equivalent SDOF System Model For Estimating The Earthquake Response of R/C Buildings With Hysteretic DampersAlex MolinaBelum ada peringkat
- Assessment - Lesson 1Dokumen12 halamanAssessment - Lesson 1Charlynjoy AbañasBelum ada peringkat
- Explorations - An Introduction To Astronomy-HighlightsDokumen10 halamanExplorations - An Introduction To Astronomy-HighlightsTricia Rose KnousBelum ada peringkat
- Urbanization As A Transformative Force: Quick FactsDokumen20 halamanUrbanization As A Transformative Force: Quick FactsJulio CovarrubiasBelum ada peringkat
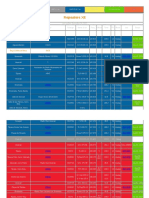
- Repeaters XE PDFDokumen12 halamanRepeaters XE PDFenzzo molinariBelum ada peringkat
- Assignment No1 of System Analysis and Design: Submitted To Submitted byDokumen7 halamanAssignment No1 of System Analysis and Design: Submitted To Submitted byAnkur SinghBelum ada peringkat
- Ariston Oven ManualDokumen16 halamanAriston Oven ManualJoanne JoanneBelum ada peringkat
- Failure CountersDokumen28 halamanFailure CountersБотирали АзибаевBelum ada peringkat
- Handouts - Entity Relationship DiagramDokumen8 halamanHandouts - Entity Relationship Diagramsecret studetBelum ada peringkat
- MA KP3-V2H-2 enDokumen155 halamanMA KP3-V2H-2 enJavier MiramontesBelum ada peringkat
- Manoj KR - KakatiDokumen5 halamanManoj KR - Kakatimanoj kakatiBelum ada peringkat
- Philippines Disaster Response PlanDokumen7 halamanPhilippines Disaster Response PlanJoselle RuizBelum ada peringkat
- Summer 2019 English Reinforcement LessonsDokumen31 halamanSummer 2019 English Reinforcement LessonsAizalonica GalangBelum ada peringkat
- Joey Cena 2Dokumen1 halamanJoey Cena 2api-635313033Belum ada peringkat
- FINAL Conflicts 2019 Official Guidelines PDFDokumen48 halamanFINAL Conflicts 2019 Official Guidelines PDFxsar_xBelum ada peringkat
- SOP For Storage of Temperature Sensitive Raw MaterialsDokumen3 halamanSOP For Storage of Temperature Sensitive Raw MaterialsSolomonBelum ada peringkat
- NUC BIOS Update Readme PDFDokumen3 halamanNUC BIOS Update Readme PDFSuny Zany Anzha MayaBelum ada peringkat
- Air India CpioDokumen5 halamanAir India CpioVicky GautamBelum ada peringkat
- JNVD Souvenir FinalDokumen67 halamanJNVD Souvenir Finalkundanno1100% (1)
- Ce QuizDokumen2 halamanCe QuizCidro Jake TyronBelum ada peringkat