Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Autodesk Knowledge Network: Skip To Main ContentDokumen8 halamanAutodesk Knowledge Network: Skip To Main ContentEA Kev RamosBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Judging Building CodesDokumen4 halamanJudging Building CodesEA Kev RamosBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
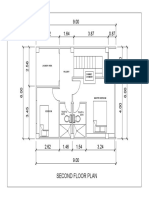
- 2ND Floor Plan MARANODokumen1 halaman2ND Floor Plan MARANOEA Kev RamosBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Quizlet Reviewer BLDG Laws 1Dokumen65 halamanQuizlet Reviewer BLDG Laws 1EA Kev RamosBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Characteristics of Colonial Style ArchitectureDokumen1 halamanCharacteristics of Colonial Style ArchitectureEA Kev RamosBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
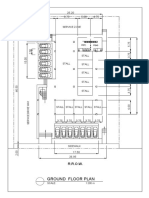
- Ground Floor PlanDokumen1 halamanGround Floor PlanEA Kev RamosBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- George Washington Bridge: FirmitasDokumen6 halamanGeorge Washington Bridge: FirmitasEA Kev RamosBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Deped School Req 2016Dokumen22 halamanDeped School Req 2016EA Kev RamosBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Bamboo TensegrityDokumen13 halamanBamboo TensegrityEA Kev RamosBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Cut Along Dotted LineDokumen1 halamanCut Along Dotted LineEA Kev RamosBelum ada peringkat
- Bamboo Research in The PhilippinesDokumen12 halamanBamboo Research in The PhilippinesEA Kev RamosBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Comparative Study On Initial Public Offer (Ipo) : Management of Indian Financial SystemsDokumen21 halamanComparative Study On Initial Public Offer (Ipo) : Management of Indian Financial SystemsHimanshu JoshiBelum ada peringkat
- AnalogyDokumen25 halamanAnalogyEA Kev RamosBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Planning 1 ReviewerDokumen3 halamanPlanning 1 ReviewerEA Kev RamosBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Principles of CompositionDokumen10 halamanThe Principles of CompositionEA Kev Ramos50% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Writing Assessment & Evaluation Rubrics PDFDokumen47 halamanWriting Assessment & Evaluation Rubrics PDFEA Kev RamosBelum ada peringkat
- 04 TP FinancialDokumen4 halaman04 TP Financialbless erika lendroBelum ada peringkat
- Suspension Mansons 2Dokumen45 halamanSuspension Mansons 2Andres Silva67% (3)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Dokumen2 halamanIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Windows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwDokumen15 halamanWindows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwYeraldo MarinBelum ada peringkat
- Playing Djembe PDFDokumen63 halamanPlaying Djembe PDFpbanerjeeBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- EpitheliumDokumen48 halamanEpitheliumdrpankaj28100% (1)
- Stock Control Management SyestemDokumen12 halamanStock Control Management SyestemJohn YohansBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Physicochemical, Phytochemical, Mineral Analysis and Invitro Anti-Oxidant Activity of Shatavari Ghrita (Polyherbal Formulation)Dokumen11 halamanPhysicochemical, Phytochemical, Mineral Analysis and Invitro Anti-Oxidant Activity of Shatavari Ghrita (Polyherbal Formulation)International Journal of Innovative Science and Research TechnologyBelum ada peringkat
- RPS Spare CatalogDokumen25 halamanRPS Spare Catalogसुरेश चंद Suresh ChandBelum ada peringkat
- HG G2 Q1 W57 Module 3 RTPDokumen11 halamanHG G2 Q1 W57 Module 3 RTPJennilyn Amable Democrito100% (1)
- Lecture Note 10 - Mortgage and Mortgage-Backed SecuritiesDokumen58 halamanLecture Note 10 - Mortgage and Mortgage-Backed Securitiesben tenBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Aficionado PERDokumen19 halamanAficionado PERMaecaella LlorenteBelum ada peringkat
- FS0008 Toolangi State Forest Walking TrailsDokumen2 halamanFS0008 Toolangi State Forest Walking TrailsMichael ConosBelum ada peringkat
- Chenrezi Sadhana A4Dokumen42 halamanChenrezi Sadhana A4kamma100% (7)
- LESSON PLAN IN wRITING A REPORTDokumen2 halamanLESSON PLAN IN wRITING A REPORTMarkaton Dihagnos100% (4)
- Eapp Las Q3 Week 1Dokumen8 halamanEapp Las Q3 Week 1Maricel VallejosBelum ada peringkat
- CWTS Narrative ReportDokumen10 halamanCWTS Narrative ReportJa Rich100% (1)
- Mechanical Engineering Research PapersDokumen8 halamanMechanical Engineering Research Papersfvfzfa5d100% (1)
- 750 Famous Motivational and Inspirational QuotesDokumen53 halaman750 Famous Motivational and Inspirational QuotesSaanchi AgarwalBelum ada peringkat
- Tesla, Inc.: Jump To Navigation Jump To Search Tesla Induction Motor AC MotorDokumen90 halamanTesla, Inc.: Jump To Navigation Jump To Search Tesla Induction Motor AC MotorEdi RaduBelum ada peringkat
- Studi Penanganan Hasil Tangkapan Purse Seine Di KM Bina Maju Kota Sibolga Study of Purse Seine Catches Handling in KM Bina Maju Sibolga CityDokumen8 halamanStudi Penanganan Hasil Tangkapan Purse Seine Di KM Bina Maju Kota Sibolga Study of Purse Seine Catches Handling in KM Bina Maju Sibolga CitySavira Tapi-TapiBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Santrock Section 1 Chapter 1Dokumen19 halamanSantrock Section 1 Chapter 1Assumpta Minette Burgos75% (8)
- Jyotsna G. Singh - Shakespeare and Postcolonial Theory (2019)Dokumen265 halamanJyotsna G. Singh - Shakespeare and Postcolonial Theory (2019)luisaBelum ada peringkat
- Technical Analysis CourseDokumen51 halamanTechnical Analysis CourseAkshay Chordiya100% (1)
- GOUSGOUNIS Anastenaria & Transgression of The SacredDokumen14 halamanGOUSGOUNIS Anastenaria & Transgression of The Sacredmegasthenis1Belum ada peringkat
- Nutrition Science by B Srilakshmi PDFDokumen6 halamanNutrition Science by B Srilakshmi PDFRohan Rewatkar46% (35)
- New Action Plan Launched To Enhance Somali Women's Role in Somalia's Maritime SectorDokumen5 halamanNew Action Plan Launched To Enhance Somali Women's Role in Somalia's Maritime SectorUNSOM (The United Nations Assistance Mission in Somalia)Belum ada peringkat
- (2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Dokumen249 halaman(2010) Formulaic Language and Second Language Speech Fluency - Background, Evidence and Classroom Applications-Continuum (2010)Như Đặng QuếBelum ada peringkat
- Halai Entu: Kohhrana Thuhril (Sermon) Chungchang - IiDokumen4 halamanHalai Entu: Kohhrana Thuhril (Sermon) Chungchang - IiRollick LalnuntluangaBelum ada peringkat
- BI410 Plant Developmental BiologyDokumen41 halamanBI410 Plant Developmental BiologyLaisla CagliariBelum ada peringkat
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (32)