Anda mungkin juga menyukai
- Supreme Court JudgementDokumen35 halamanSupreme Court Judgementdmurali73Belum ada peringkat
- Practice Letters A ZDokumen26 halamanPractice Letters A Zsm1234@att.netBelum ada peringkat
- Fields in NeuroophthalDokumen14 halamanFields in Neuroophthaldmurali73Belum ada peringkat
- CT-1000 Corneal TopographerDokumen1 halamanCT-1000 Corneal Topographerdmurali73100% (1)
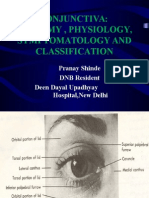
- Conjunctivaanatomyandphysiology 140805084207 Phpapp02Dokumen32 halamanConjunctivaanatomyandphysiology 140805084207 Phpapp02dmurali73Belum ada peringkat
- Content ServerDokumen4 halamanContent Serverdmurali73Belum ada peringkat
- Teaching Aids DR DMKDokumen56 halamanTeaching Aids DR DMKdmurali73Belum ada peringkat
- 2010HMF MS32 PDFDokumen2 halaman2010HMF MS32 PDFdmurali73Belum ada peringkat
- Mata Malignant Eyelid TumoursDokumen17 halamanMata Malignant Eyelid Tumoursmuhammad fajrinBelum ada peringkat
- ImageCLASS MF3010 - Canon India - PersonalDokumen2 halamanImageCLASS MF3010 - Canon India - Personaldmurali73Belum ada peringkat
- Sankara Nethralaya Clinical Practice Patterns in OPHTHALMOLOGYDokumen452 halamanSankara Nethralaya Clinical Practice Patterns in OPHTHALMOLOGYjordi28098380% (5)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Occupational Safety and Health Guidance Manual For Hazardous Waste Site ActivitiesDokumen142 halamanOccupational Safety and Health Guidance Manual For Hazardous Waste Site ActivitiesMarcelo Gil SimõesBelum ada peringkat
- Forcep DeliveryDokumen32 halamanForcep DeliverybbaltazarjaniceBelum ada peringkat
- Urine Culture Manual MT - SINAI PDFDokumen15 halamanUrine Culture Manual MT - SINAI PDFAvi VermaBelum ada peringkat
- Thalassemia in Iraq Review Article: AbstractDokumen4 halamanThalassemia in Iraq Review Article: AbstractRana RaedBelum ada peringkat
- Rarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMDokumen13 halamanRarwrmicroscopic Examination of Urine: RCF 1.118 X 10 XR CMXRPMpixiedustBelum ada peringkat
- E.coli SmitaDokumen40 halamanE.coli SmitaNeha SinhaBelum ada peringkat
- ArthrocentesisDokumen10 halamanArthrocentesisPranave PBelum ada peringkat
- Frist Aid PPT For Pharm PDFDokumen257 halamanFrist Aid PPT For Pharm PDFAbdulwhab MohammedBelum ada peringkat
- Azithromycin Drug StudyDokumen2 halamanAzithromycin Drug StudySHEILA MAE SACLOTBelum ada peringkat
- Department of HealthDokumen2 halamanDepartment of HealthdenBelum ada peringkat
- Hiatal HerniaDokumen13 halamanHiatal HerniaDerrick SHEMABelum ada peringkat
- Kanski'S: Clinical OphthalmologyDokumen453 halamanKanski'S: Clinical OphthalmologyMohin hossain100% (1)
- CE (Arnp) F (SH) PF1 (AG KM) PFA (AG KM) PN (KM)Dokumen4 halamanCE (Arnp) F (SH) PF1 (AG KM) PFA (AG KM) PN (KM)Sachintha WijesiriwardhanaBelum ada peringkat
- Literature Review Panic DisorderDokumen7 halamanLiterature Review Panic Disorderafmzwgeabzeksp100% (1)
- WANDERING - ICD-9 Sample Letter - SUPPORT NEEDEDDokumen2 halamanWANDERING - ICD-9 Sample Letter - SUPPORT NEEDEDautismoneBelum ada peringkat
- Guidelines For Malaria Vector Control in Malaysia Tahun 2022Dokumen78 halamanGuidelines For Malaria Vector Control in Malaysia Tahun 2022Nur Fatihah ShaharuddinBelum ada peringkat
- English For Careers Medicine 2 Student's BookDokumen145 halamanEnglish For Careers Medicine 2 Student's BookSt87% (15)
- (F1) Headache PDFDokumen66 halaman(F1) Headache PDFmdBelum ada peringkat
- POCUSDokumen10 halamanPOCUSSMIBA MedicinaBelum ada peringkat
- Arup Kumar Kundu-Bedside Clinics in Medicine, Part 2, 5 - E-Academic Publishers (2010)Dokumen355 halamanArup Kumar Kundu-Bedside Clinics in Medicine, Part 2, 5 - E-Academic Publishers (2010)kumar90% (10)
- Demands for Grants 2021-22 for Ministry of Health and Family WelfareDokumen10 halamanDemands for Grants 2021-22 for Ministry of Health and Family WelfareAshish KumarBelum ada peringkat
- Problems and Disadvantages of The Introduction of Modern Medicine in The Turkestan Governor-GeneralDokumen9 halamanProblems and Disadvantages of The Introduction of Modern Medicine in The Turkestan Governor-GeneralResearch ParkBelum ada peringkat
- Jama Ference 2020 It 200013Dokumen2 halamanJama Ference 2020 It 200013miguelalmenarezBelum ada peringkat
- Anesthetic Consideration For Patients With Obstructive JaundiceDokumen47 halamanAnesthetic Consideration For Patients With Obstructive JaundiceagatakassaBelum ada peringkat
- Test Your Nursing Knowledge: CA1 Module 3 ActivitiesDokumen6 halamanTest Your Nursing Knowledge: CA1 Module 3 ActivitiesEsmareldah Henry SirueBelum ada peringkat
- 1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-ConceptionDokumen2 halaman1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-Conceptionjoel TorresBelum ada peringkat
- Raport de Autoevaluare 2008Dokumen90 halamanRaport de Autoevaluare 2008Mara GonceaBelum ada peringkat
- Silent Reflux SymptomsDokumen2 halamanSilent Reflux Symptomsu3dejce896Belum ada peringkat
- Lidocaine Mechanism of Action, Indications, Contraindications and Side EffectsDokumen14 halamanLidocaine Mechanism of Action, Indications, Contraindications and Side EffectsJennyLapitan100% (2)
- Cough - Wikipedia PDFDokumen59 halamanCough - Wikipedia PDFSrinivasreddy G Maali PatelBelum ada peringkat