Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Orange SurgeryDokumen3 halamanOrange SurgeryMichele Fantin100% (1)
- Cell Transport WorksheetDokumen3 halamanCell Transport WorksheetDat White Boi Player20% (1)
- Clinical Pediatric NotesDokumen132 halamanClinical Pediatric Notessphadungkit100% (3)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hijaamah (Cupping Therapy) As Therapy and Medicine: October 31, 2012 at 4:26pmDokumen17 halamanHijaamah (Cupping Therapy) As Therapy and Medicine: October 31, 2012 at 4:26pmShamil Jamaldeen100% (1)
- Fracture Healing and Bone RemodellingDokumen1 halamanFracture Healing and Bone RemodellingFarhan IzaniBelum ada peringkat
- DDZDokumen4 halamanDDZFarhan IzaniBelum ada peringkat
- Semester 3 Haemopoietic & Lymphatic System: AnatomyDokumen11 halamanSemester 3 Haemopoietic & Lymphatic System: AnatomyFarhan IzaniBelum ada peringkat
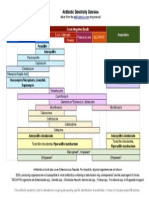
- Antibiotic Sensitivity Overview for Gram Positive Cocci, Gram Negative Bacilli and AnaerobesDokumen1 halamanAntibiotic Sensitivity Overview for Gram Positive Cocci, Gram Negative Bacilli and AnaerobesGuillermo Damian RodriguezBelum ada peringkat
- CNS Anatomy, Physiology, Biochemistry, Pathology, Microbiology, Pharmacology & ParasitologyDokumen1 halamanCNS Anatomy, Physiology, Biochemistry, Pathology, Microbiology, Pharmacology & ParasitologyFarhan IzaniBelum ada peringkat
- Global Asthma Report 2011Dokumen76 halamanGlobal Asthma Report 2011Farhan IzaniBelum ada peringkat
- Pneumonia and Respiratory Tract Infections in ChildrenDokumen37 halamanPneumonia and Respiratory Tract Infections in ChildrenjayasiinputBelum ada peringkat
- Mazda3 Digital BrochureDokumen28 halamanMazda3 Digital BrochureFarhan IzaniBelum ada peringkat
- Measure The Strap and See The FitDokumen1 halamanMeasure The Strap and See The FitFarhan IzaniBelum ada peringkat
- All New Mazda2 Digital BrochureDokumen23 halamanAll New Mazda2 Digital BrochureFarhan IzaniBelum ada peringkat
- General Medicine 500 Case Study PDFDokumen22 halamanGeneral Medicine 500 Case Study PDFFarhan IzaniBelum ada peringkat
- Clinical Medicine II ASTHMADokumen17 halamanClinical Medicine II ASTHMAFarhan IzaniBelum ada peringkat
- Upper Respiratory Infection Case (1) .EdDokumen3 halamanUpper Respiratory Infection Case (1) .EdFarhan IzaniBelum ada peringkat
- November 2015: Sunday Monday Tuesday Wednesday Thursday Friday Saturday 1 2 3 4 5 6 7Dokumen2 halamanNovember 2015: Sunday Monday Tuesday Wednesday Thursday Friday Saturday 1 2 3 4 5 6 7Farhan IzaniBelum ada peringkat
- Shell ScholarshipDokumen2 halamanShell ScholarshipThuran NathanBelum ada peringkat
- How Do Phagocytes Work in The BodyDokumen2 halamanHow Do Phagocytes Work in The Bodykei04086100% (1)
- Critical Hits Reference SheetDokumen6 halamanCritical Hits Reference Sheetknight.errantBelum ada peringkat
- New Ballard Score Overview: An Enhanced Tool for Assessing Gestational Age in Premature InfantsDokumen11 halamanNew Ballard Score Overview: An Enhanced Tool for Assessing Gestational Age in Premature Infantsdr_alfuBelum ada peringkat
- Benign Prostatic Hyperplasia: A Case Analysis OnDokumen70 halamanBenign Prostatic Hyperplasia: A Case Analysis OnAngelica RelanaBelum ada peringkat
- Science4 - Q2 - Mod1 - Major Organs of The Human Body - Version3Dokumen50 halamanScience4 - Q2 - Mod1 - Major Organs of The Human Body - Version3Glaiza RomeroBelum ada peringkat
- Cell (XI Grade)Dokumen27 halamanCell (XI Grade)Ahmad LuthfyBelum ada peringkat
- OtotoxicityDokumen233 halamanOtotoxicityGianluca Gandini100% (1)
- ASJA BOYS’ COLLEGE END OF TERM EXAMDokumen16 halamanASJA BOYS’ COLLEGE END OF TERM EXAMYɵʉňğ ĢênnäBelum ada peringkat
- Connective Tissue StainsDokumen42 halamanConnective Tissue StainsSMBelum ada peringkat
- Transport in AnimalsDokumen81 halamanTransport in AnimalsIbrahim NOORZADBelum ada peringkat
- Growth Assessment ParametersDokumen97 halamanGrowth Assessment ParametersAurthi ElamparithiBelum ada peringkat
- Respiratory Assessment LandmarksDokumen15 halamanRespiratory Assessment LandmarksChilled Moo MooBelum ada peringkat
- Hematology 2 LaboratoryDokumen11 halamanHematology 2 LaboratoryChristine BadilloBelum ada peringkat
- 101 2017 3 B PDFDokumen18 halaman101 2017 3 B PDFPasipanodya MuzendaBelum ada peringkat
- Cosmtic Diploma SyllabusDokumen11 halamanCosmtic Diploma SyllabusPrakash VerekarBelum ada peringkat
- Polygraphy ReviewDokumen129 halamanPolygraphy ReviewKAPITAN TUMBABelum ada peringkat
- IHM Manual VTCTDokumen57 halamanIHM Manual VTCTEnvie AestheticsBelum ada peringkat
- Medico Legal Report - ThamaeDokumen13 halamanMedico Legal Report - ThamaencetaniBelum ada peringkat
- 20 - Pediatric Urinary DisordersDokumen62 halaman20 - Pediatric Urinary DisordersKhaalid AbdirahmanBelum ada peringkat
- Pathoma BreastDokumen8 halamanPathoma BreastLauren LaMonicaBelum ada peringkat
- Accessory Organ of The AbdomenDokumen58 halamanAccessory Organ of The AbdomenOgundipe olorunfemiBelum ada peringkat
- Optha Eyelids Orbit Lacrimal DR - Hernando L. Cruz JRDokumen11 halamanOptha Eyelids Orbit Lacrimal DR - Hernando L. Cruz JRJack Ortega PuruggananBelum ada peringkat
- Q2 - First Summative TestDokumen3 halamanQ2 - First Summative TestMilagros ReyesBelum ada peringkat
- Ch 26: Components and Functions of the Urinary SystemDokumen17 halamanCh 26: Components and Functions of the Urinary SystemgopscharanBelum ada peringkat
- EXPERIMENT 10 External Anatomy of The FROGDokumen6 halamanEXPERIMENT 10 External Anatomy of The FROGoinkBelum ada peringkat
- Joint Clinico-Pathologic Conference: October 3, 2008Dokumen50 halamanJoint Clinico-Pathologic Conference: October 3, 2008ianjohn724Belum ada peringkat
- A Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFDokumen7 halamanA Histopathological Study of Liver in 118 Cases of Cirrhosis 2167 0889 1000193 PDFHemin HassanBelum ada peringkat