Measuring The Glycemic Index of Foods, Interlaboratory Study
Diunggah oleh
Guillermo Martinez GarciaJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Measuring The Glycemic Index of Foods, Interlaboratory Study
Diunggah oleh
Guillermo Martinez GarciaHak Cipta:
Format Tersedia
Measuring the glycemic index of foods: interlaboratory study15
Thomas MS Wolever, Jennie C Brand-Miller, John Abernethy, Arne Astrup, Fiona Atkinson, Mette Axelsen,
Inger Bjrck, Furio Brighenti, Rachel Brown, Audrey Brynes, M Cristina Casiraghi, Murielle Cazaubiel,
Linda Dahlqvist, Elizabeth Delport, Gareth S Denyer, Daniela Erba, Gary Frost, Yvonne Granfeldt, Shelagh Hampton,
Valerie A Hart, Katja A Hatnen, C Jeya Henry, Steve Hertzler, Sarah Hull, Johann Jerling, Kelly L Johnston,
Helen Lightowler, Neil Mann, Linda Morgan, Leonora N Panlasigui, Christine Pelkman, Tracy Perry,
Andreas FH Pfeiffer, Marlien Pieters, D Dan Ramdath, Rayna T Ramsingh, S Daniel Robert, Carol Robinson,
Essi Sarkkinen, Francesca Scazzina, Dave Clark D Sison, Birgitte Sloth, Jane Staniforth, Niina Tapola, Liisa M Valsta,
Inge Verkooijen, Martin O Weickert, Antje R Weseler, Paul Wilkie, and Jian Zhang
KEY WORDS
Clinical trial, humans, dietary carbohydrate,
glycemic index, glucose, methodology
INTRODUCTION
The glycemic index (GI) is a measure of the blood glucoseraising ability of the available carbohydrate in foods defined as
the incremental area under the glycemic response curve (AUC)
elicited by a portion of food containing 50 g available carbohydrate expressed as a percentage of the AUC elicited by 50 g
glucose in the same subject. Prospective studies suggest that
low-GI diets may reduce the risk of diabetes (1, 2), cardiovascular disease (3, 4), metabolic syndrome (5), chronic inflammation (6), and possibly some types of cancer (712). Clinical trials
have shown that low-GI diets improve glycemic control in diabetes (13), increase insulin sensitivity (14, 15) and -cell function (16, 17), reduce food intake (18) and body weight (19 21),
influence memory (22, 23), and may reduce serum cholesterol
(24). Diabetes associations in the United Kingdom (25), Canada
(26), Australia (27), Europe (28), and the United States (29)
indicate that GI is a useful tool for differentiating between carbohydrates. For these reasons, labeling of GI on foods has been
proposed or is already occurring in Australia, South Africa, Sweden, United Kingdom, and Germany, with several commercial
laboratories measuring the GI of foods.
For regulatory purposes, an approved method of measuring
the GI of foods is required, and standards must be developed to
1
From the Department of Nutritional Sciences, University of Toronto and
Glycemic Index Laboratories, Inc, Toronto, Ontario, Canada (TMSW); the
Human Nutrition Unit, Department of Biochemistry, University of Sydney,
Sydney, NSW, Australia (JCB-M, FA, and GSD); AMK Research, Inc,
Gainsville, FL, USA (JA); the Department of Human Nutrition, Centre for
Advanced Food Studies, Faculty of Life Sciences, University of Copenhagen, Frederiksberg, Denmark (AA and BS); the Department of Clinical
Nutrition, Gothenburg University, Gothenburg, Sweden (MA and LD); the
Centre for Chemistry and Chemical Engineering, Lund University, Lund,
Sweden (IB and YG); the Human Nutrition Unit, Department of Public
Health, University of Parma, Parma, Italy (FB and FS); the Department of
Human Nutrition, University of Otago, Dunedin, New Zealand (RB and TP);
the Nutrition and Dietetic Department, Hammersmith Hospital, Imperial
College, London, United Kingdom (AB and GF); DiSTAM - Nutrition Unit,
University of Milan, Milan, Italy (MCC and DE); Biofortis, Nantes, France
(MC); the GI Foundation of South Africa, Mpumalanga, South Africa (ED);
the Faculty of Health and Medical Sciences, University of Surrey, Guildford,
Surrey, United Kingdom (SHampton, KLJ, and LMorgan); the Nutrition
Unit, Department of Health Promotion and Chronic Disease Prevention,
National Public Health Institute (KTL), Helsinki, Finland (KH and LMV);
the School of Life Sciences, Oxford Brookes University, Oxford, United
Am J Clin Nutr 2008;87(suppl):247S57S. Printed in USA. 2008 American Society for Nutrition
247S
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
ABSTRACT
Background: Many laboratories offer glycemic index (GI) services.
Objective: We assessed the performance of the method used to
measure GI.
Design: The GI of cheese-puffs and fruit-leather (centrally provided) was measured in 28 laboratories (n 311 subjects) by using
the FAO/WHO method. The laboratories reported the results of their
calculations and sent the raw data for recalculation centrally.
Results: Values for the incremental area under the curve (AUC)
reported by 54% of the laboratories differed from central calculations. Because of this and other differences in data analysis, 19% of
reported food GI values differed by 5 units from those calculated
centrally. GI values in individual subjects were unrelated to age, sex,
ethnicity, body mass index, or AUC but were negatively related to
within-individual variation (P 0.033) expressed as the CV of the
AUC for repeated reference food tests (refCV). The betweenlaboratory GI values (mean SD) for cheese-puffs and fruit-leather
were 74.3 10.5 and 33.2 7.2, respectively. The mean laboratory
GI was related to refCV (P 0.003) and the type of restrictions on
alcohol consumption before the test (P 0.006, r2 0.509 for
model). The within-laboratory SD of GI was related to refCV (P
0.001), the glucose analysis method (P 0.010), whether glucose
measures were duplicated (P 0.008), and restrictions on dinner the
night before (P 0.013, r2 0.810 for model).
Conclusions: The between-laboratory SD of the GI values is 9.
Standardized data analysis and low within-subject variation (refCV
30%) are required for accuracy. The results suggest that common
misconceptions exist about which factors do and do not need to be
controlled to improve precision. Controlled studies and cost-benefit
analyses are needed to optimize GI methodology. The trial was
registered at clinicaltrials.gov as NCT00260858.
Am J Clin
Nutr 2008;87(suppl):247S57S.
248S
WOLEVER ET AL
TABLE 1
Composition of the test foods
Cheese Puffs
Fruit Leather3
Weight
Fat
Protein
Total CHO1
Dietary fiber
Available CHO
82.4
63.6
15.1
0.0
6.1
0.0
54.5
54.5
4.5
4.5
50.0
50.0
CHO, carbohydrate.
Pirates Booty, Roberts American Gourmet, Sea Cliff, NY.
3
Original Sweet Strawberry flavor, Stretch Island Fruit Co, Allyn, WA.
2
Kingdom (CJH and HL); the Department of Human Nutrition, Ohio State
University, Columbus, OH (SHertzler and PW); the Nutrition and Health
Section, Leatherhead Food International, Surrey, United Kingdom (SHull);
the Department of Nutrition, Northwest University, Potchefstroom, South
Africa (JJ and MP); the International Diabetes Institute, Melbourne, Victoria,
Australia (NM and CR); Reading Scientific Services, Ltd, Reading, Berks,
United Kingdom (VAH and JS); the College of Home Economics, University
of the Philippines, Diliman, The Philippines (LP and DCDS); the Department
of Exercise and Nutrition Sciences, University at Buffalo, Buffalo, NY (CP);
the Department of Clinical Nutrition, German Institute of Human Nutrition
(DIFE) Potsdam-Rehbruecke, Nuthetal, and the Department of Endocrinology, Diabetes and Nutrition, Charit-University-Medicine Berlin, Germany
(AFHP and MOW); the Biochemistry Unit, Department of Preclinical Sciences, Faculty of Medical Sciences, The University of the West Indies, St
Augustine, Trinidad and Tobago (DDR and RTR); the Program in Dietetics,
School of Health Sciences , Health Campus, Universiti Sains Malaysia,
Kelantan, Malaysia (SDR); Oy Foodfiles Ltd, Kuopio, Finland (ES and NT);
NutriScience BV, Maastricht, Netherlands (IV and AW); and the Institute of
Nutrition and Food Safety, Chinese Center for Disease Control and Prevention, Beijing, China (JZ).
2
Presented at an ILSI Europe workshop titled Glycemic Response and
Health, held in Nice, France, on 6-8 December 2006.
3
Supported by Glycaemic Index Testing, Inc, Toronto, ON, Canada;
Sydney University GI Research Services, University of Sydney; ILSI Europe, Brussels, Belgium; Biofortis; Department of Human Nutrition, University of Otago; Philippine Council for Health Research and Development,
Department of Science and Technology, University of the Philippines; GI
Expert Laboratory, Lund, Sweden; GI Foundation of South Africa; GI Laboratories, Inc; GI Testing Services, Oxford Brookes University; Hammersmith Food Research; University of Surrey; International Diabetes Institute;
Leatherhead Food International; Ministry of Agriculture and Forestry, Academy of Finland, National Public Health Institute, Finland; Reading Scientific
Services, Ltd; NutriScience BV; Oy Foodfiles, Ltd; University of Parma;
Universiti Sains Malaysia; and University of the West Indies.
4
Address reprint requests to ILSI Europe. E-mail: publications@
ilsieurope.be.
5
Address correspondence to T Wolever, Department of Nutritional Sciences, University of Toronto, Toronto, Ontario M5S 3E2, Canada. E-mail:
thomas.wolever@utoronto.ca.
variation of the means and SDs of GI values measured by different laboratories around the world and to determine the extent
to which sources of methodologic variation may explain the
interlaboratory variation of GI means and SD.
MATERIALS AND METHODS
Each participating laboratory was sent 3 food products for GI
determination: an oat biscuit, cheese puffs, and fruit leather (Table 1). As the result of a misunderstanding about the definition of
the term available carbohydrate between the investigators and
the manufacturer, it was subsequently learned that the portion
size of the oat biscuit used contained 40% more available carbohydrate than expected, and so the results for this food are not
included here. The foods were chosen because they were readyto-eat, and preliminary data suggested that one would have a high
GI (70) and the other a low GI (55). The protocol indicated
that 10 healthy subjects should be studied in each location, but
some laboratories included up to 14 subjects. The subjects were
males and nonpregnant, nonlactating females aged 18 75 y who
did not have diabetes. The protocol used by each location was
approved by a human subjects ethics review committee, and each
participating subject provided informed consent by signing an
approved consent form.
In each location, the subjects were studied on 35 separate
occasions in the morning after they had fasted overnight. On 2
occasions, they consumed test meals consisting of one of the test
foods, and on the other occasions, the test meal consisted of the
reference food. On each occasion, after a fasting blood sample
was taken, the subjects ate the test meal and had further blood
samples drawn at 15, 30, 45, 60, 90, and 120 min after starting to
eat. The protocol indicated that capillary blood should be obtained by finger-prick, but one site obtained venous blood from
a forearm vein, and one site obtained capillary blood from the
earlobe.
The portion size of each test food contained 50 g available
carbohydrate (defined as total carbohydrate minus dietary fiber)
based on the information on the nutrition information panel. To
avoid misunderstanding about the definition of the terms on the
food label, all sites were advised about the portion sizes of the test
foods to be used. The reference food could be 50 g anhydrous
glucose, 55 g dextrose (glucose-monohydrate), or 50 g available
carbohydrate from white bread. Each laboratory determined the
number of times the reference food was tested by each subject.
The protocol indicated that each test meal was to be served with
250 to 500 mL water or tea (50 mL milk was allowed if desired).
Each subject could choose the volume and type of drink desired,
but the drink chosen was the same for all test meals consumed by
that subject. Most sites restricted the drink to only water, and one
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
enable assessment of the performance of the laboratories. The
effect of some methodologic variables on GI values is known,
and a recommended method is available (30, 31). However, the
method does not address all common methodologic variations. A
previous interlaboratory study suggested that the betweenlaboratory SD of average GI values of the same food determined
in 8 10 subjects was 9 (32). However, too few centers were
involved (n 7) to reliably assess the extent of variation in
methodology in different laboratories around the world and the
effects of such variables on the results obtained. In addition, the
extent of variation in data analysis by individual laboratories was
not assessed, because all calculations were performed centrally.
Thus, the purposes of this study were to assess the magnitude of
249S
GLYCEMIC INDEX INTERLABORATORY STUDY
TABLE 2
Characteristics of the subjects studied
Males/females (n)
Age (y)
Height (cm)
Weight (kg)
BMI (kg/m2)
Underweight [n (%)]
Ideal weight [n (%)]
Overweight [n (%)]
Obese [n (%)]
Reference AUC (mmol min/L)3
Reference CV (%)
Glycemic index (%)4
White
(n 241)
Other
(n 70)1
101/140
30.0 0.72
172 1
69.9 0.9
23.4 0.2
4 (2)
176 (73)
51 (21)
10 (4)
206 5
22.3 1.0
53.1 1.2
26/44
28.7 1.1
163 1
60.3 1.4
22.6 0.4
2 (3)
43 (61)
21 (30)
4 (5)
258 13
23.1 2.9
53.8 2.4
NS
NS
0.0001
0.0001
0.090
NS
0.0001
NS
NS
26 Southeast-Asian, 21 East-Asian, 16 South-Asian, 3 mixed African/
South-Asian, 3 African, and 1 Middle-Eastern.
2
x SEM (all such values).
3
Mean area under the curve for reference food; values for white bread
were adjusted by dividing by 0.71.
4
Mean glycemic index of 2 test foods for 287 subjects who tested both
foods.
the mean plus 2 SDs were considered to be outliers and were
excluded from the final results.
Individual AUC and GI values for the 2 test foods were compared by analysis of variance (ANOVA) for a 2-factor experiment with repeated measures on one factor (35) examining the
main effects of laboratory and food and the laboratory food
interaction. The influence of laboratory methods on laboratory
mean and SD of the GI values was determined by step-wise
multiple regression analysis (Lotus 1-2-3 97 Edition; Lotus Development Corp;, Cambridge, MA) by using the step-up procedure described by Snedecor and Cochran (36). For regression
analysis involving subject variables, dummy values were used
for sex (F 0, M 1) and ethnicity (white 0, other 1). For
regression analysis involving methodologic variables, the methods used at each laboratory were placed into 2 to 4 categories,
depending on the range of methods used, and dummy values
between 0 and 3 were assigned to the categories in order of the
unadjusted means within the categories. Information about the
use of duplicate blood samples and duplicate measurements of
glucose was collapsed into a single category whether any duplication was done or not.
RESULTS
A total of 314 subjects were involved in the study, of whom 2
dropped out and 1 was excluded for being discovered to have
impaired glucose tolerance. Of the 311 who were included, 241
(77%) were white, 26 were Southeast-Asian, 21 were EastAsian, 16 were South-Asian, 3 were African, 3 were mixed
African/South-Asian, and 1 was Middle-Eastern (Table 2). The
white subjects did not differ significantly from the others in sex
or age, but were significantly taller and heavier; however, the
difference in BMI was not significant. The glycemic response
elicited by the reference food was significantly less in the white
subjects than in the others (Table 2), but the reference CV and
mean GI values did not differ significantly. Fourteen laboratories
provided information about the subjects medication use; of the
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
allowed coffee as a choice. Test meals were consumed within 10
min. Timing for blood samples started with the first bite of the test
meal.
Each laboratory could measure glucose in whole blood,
plasma, or serum by any recognized method, as long as the
method used was the same for all tests. The incremental area
under the glucose response curve (AUC) above the fasting glucose concentration, ignoring the area beneath the fasting concentration, was calculated by using the trapezoid rule. The AUC
of each subject after each test food was expressed as a percentage
of the mean AUC elicited by the reference food in the same
subject. The mean of these values for all the subjects was the food
GI. If white bread was used as the reference food, the GI values
were multiplied by 0.71 to convert them to the glucose scale (ie,
the GI of glucose 100).
Participating laboratories were asked to send the following
information about their methods and results to the central laboratory (University of Toronto): inclusion and exclusion criteria
for subjects; the reference food used; the method used to sample
blood and measure glucose; whether measures of glucose were
repeated; the restrictions (if any) placed on subjects with respect
to exercise, alcohol consumption, smoking, length of fasting, and
the meal consumed the evening before each test; the drink served
with the test meal; the age, sex, ethnicity, height, weight, and
body mass index (BMI; in kg/m2) of each subject; medications
used by subjects (if any); glucose concentrations at each time
point; AUC values calculated locally for each test meal taken by
each subject; and the mean and SD of the GI values calculated
locally.
The adiposity of white subjects was classified as underweight,
ideal weight, overweight, or obese by using BMI cutoffs of
18.5, 18.525.0, 25.130.0, and 30.0, respectively. Because,
for a given BMI, South and East Asians have more body fat than
do whites (33), nonwhite subjects were classified as underweight, ideal weight, overweight, or obese by using BMI cutoffs
of 18.0, 18.0 23.0, 23.126.9, and 26.9.
The mean and SD of the AUC and GI values reported by each
laboratory were compared with those calculated at the central
laboratory by using the procedure of Bland and Altman (34). The
critical value for this procedure is termed limits of agreement,
defined as the mean 2 SD of the differences between the
results using 2 different methods (in this case, the values reported
by each laboratory and the respective values calculated by the
central laboratory); thus, the limits of agreement represent the
range within which 95% of the differences lie. Limits of agreement for AUC 2 mmolmin/L and for mean GI 1.0 were
considered to be due to rounding and, therefore, insignificant;
larger values were considered to be due to calculation or reporting errors. Because significant differences were found between
reported and centrally calculated values for AUC and GI, centrally calculated AUC and GI values were used for further statistical analysis. The mean and CV (CV 100 SD/mean) of
the AUC values for repeated reference food tests were calculated
for each subject, and the results were termed reference AUC and
reference CV (refCV), respectively (CV could be calculated only
for the 26 laboratories in which the reference food was tested
more than once by each subject).
GI values were calculated by expressing each subjects AUC
after the test food as a percentage of the same subjects mean
reference AUC. The mean of the resulting values was the GI of
the food. Within each laboratory, individual values greater than
250S
WOLEVER ET AL
150 subjects at these laboratories, 30 reported taking medications, the most common of which was the oral contraceptive pill
(n 18). Other medications were angiotensin-converting enzyme inhibitors (n 3), nonsteroidal anti-inflammatory agents
(n 3), thyroid replacement therapy (n 2), and one subject
each for aspirin, -blocker, anti-histamine, antibiotic, and a
triptan for migraines. Information about the subjects smoking
habits was provided by 12 laboratories, and of the 136 subjects
involved, 3 were smokers. At 26 of the 28 participating laboratories, all subjects (n 275) tested both test foods. In the 27th
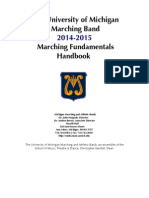
FIGURE 2. Mean blood glucose responses elicited by the reference food, cheese puffs (), and fruit leather () in 24 laboratories (n 271 subjects) that
used glucose (F) as the reference food (left) and in 4 laboratories (n 70 subjects) that used white bread (E) as the reference food.
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
FIGURE 1. A: Differences between reported and centrally calculated
individual area under the curve (AUC) values. Values are mean SD. The
scale for values represented by open squares (right y axis) is 10 times that for
values represented by closed circles (left y axis). B: The difference between
reported and centrally calculated mean glycemic index (GI) values for 2
foods plotted against the mean of the reported and centrally calculated values.
The dotted lines represent the differences in GI that are considered to be large,
which were arbitrarily chosen to be 5.
laboratory, 18 subjects were involved, 4 of whom tested both test
foods. In the 28th laboratory, 19 subjects were involved, 3 of
whom tested both foods.
Some or all of the AUC values reported by 14 (54%) of the 26
laboratories that reported AUC values to the central laboratory
were considered to be calculated or reported incorrectly (Figure
1A). The limits of agreement for 10 of these laboratories were
relatively small, ranging from 5 to 21 mmolmin/L; but for 4
of the laboratories, the limits of agreement were 50
mmol min/L. One of the latter laboratories appeared to have
reported total AUC values instead of incremental AUC. One
laboratory did not report AUC or GI values. A total of 52 mean
GI values were reported to the central laboratory (2 foods tested
in 26 laboratories); of these, 23 (44%) differed from those calculated by the central laboratory by 1 (Figure 1B). Ten (19%)
of the mean GI values differed from those calculated by the
central laboratory by 5, with at least one difference of 5 being
reported by 7 (27%) of the laboratories. These differences were
due, at least in part, to the use of different exclusion criteria by
most laboratories; 25 laboratories did not exclude any outliers
when reporting mean GI values, 2 laboratories excluded values
2 SDs from the mean, and one laboratory excluded values
10.1 and 99.9. When outliers were not excluded by the central laboratory, mean GI values calculated by the central laboratory differed by 5 from those reported by the laboratories for 9
foods reported by 4 different laboratories. One of these laboratories was the one that excluded values 10.1 and 99.9, but the
other 3 laboratories did not exclude any values. Thus, the difference in reported GI was not due to differences in exclusion
criteria for these 3 laboratories.
Individual values for mean AUC (mean of test and reference
foods) varied from 23 to 413 mmolmin/L. By stepwise multiple
regression analysis, the individual values for AUC were not
related to sex or age but were significantly related to ethnicity
(lower in white subjects than in others, P 0.001) and BMI (P
0.031; positive relation), with the combined r2 0.095. By
stepwise multiple regression analysis, the individual values for
refCV were negatively related to the mean AUC values (r2
0.017, P 0.033), but were not related to sex, ethnicity, age, or
BMI with the use of either simple (univariate) or multiple regression analysis. GI values of the individual subjects were positively related to refCV (r 0.143, P 0.020), but were not
related to sex, ethnicity, age, BMI, or mean AUC with the use of
either univariate or multiple regression analysis.
GLYCEMIC INDEX INTERLABORATORY STUDY
251S
FIGURE 3. A: Incremental area under the glycemic response curve
(AUC) elicited by the reference food in different labs. B: Coefficient of
varation (CV, where CV 100 SD/mean) of the AUC values elicited by
the reference food (tested 23 times by each subject) in different laboratories.
Values are the mean SEM for glucose (F, n 22) and white bread (E, n
4; AUC values for white bread were divided by 0.71). Open diamonds
represent the mean SEM for the 26 laboratories (reference CV could only
be calculated for the 26 laboratories that tested the reference food more than
once in each subject).
The blood glucose responses of the 2 test foods were similar
in the 24 laboratories that used glucose as the reference food
compared with the 4 that used white bread (Figure 2). The mean
AUC for the reference food (values for white bread adjusted
to the glucose scale) differed significantly between laboratories
(F (25, 301) 4.39, P 0.001; one subject with an AUC of 666
mmolmin/L was excluded as an outlier; Figure 3A). In addition,
the mean within-subject CV for the repeated reference food tests
(refCV) differed in the different laboratories (F (25, 299) 2.42,
P 0.001, Figure 3B; 2 subjects with CV 141% were excluded
as outliers). The mean adjusted AUC and refCV values for the 4
laboratories that used white bread as the reference were not
significantly different from those laboratories that used glucose
(Figure 3).
GI values for cheese puffs were available in 300 subjects, of
whom 5 were outliers (2 SDs above the laboratory mean) and
for fruit leather in 298 subjects of whom 8 were 2 SDs above
the mean. Thus, of the 598 individual GI values, 13 (2.2%) were
considered outliers and were excluded. By ANOVA, there was a
significant main effect of food (F (1, 237) 476, P 0.001), with
the mean GI of fruit leather being significantly less than that for
cheese puffs (Figures 4, A and B). The main effect of laboratory
was not significant (F (25, 249) 1.529, P 0.056), and there was
no significant food laboratory interaction (P 0.43). The
mean SD of the 28 laboratory mean GI values for cheese puffs
FIGURE 4. Mean and SD of glycemic index (GI) values from the 28
laboratories for cheese puffs (A and C, respectively) and fruit leather (B and
D, respectively). Closed circles are for laboratories using glucose as the
reference food; open circles are for laboratories using white bread as the
reference food, and the open diamond represents the mean and SD of the
values from the 28 laboratories.
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
and fruit leather, respectively, were 74.3 10.5 (Figure 4A) and
33.2 7.2 (Figure 4B). The SDs of the GI values in the 28
laboratories varied from 14 to 48 for cheese puffs (meanSD,
27.5 9.0; Figure 4C) and from 9 to 25 for fruit leather (14.7
4.2, Figure 4D).
Methodologic variables related to the test meal included the
type of reference food used, the number of reference food tests
done by each subject, and the nature of the drink given with the
test meal. By ANOVA, the variation in these factors was not
associated with any significant differences in adjusted reference
AUC, refCV, mean GI, or SD of GI (Table 3).
The laboratories varied in the methods used for blood sampling and glucose analysis. The laboratories (n 4) that took 2
fasting blood samples and used the average measure to calculate
GI tended to have a lower mean refCV and mean GI (not significant) and a significantly lower SD (Table 4). Duplicate measurement of glucose also tended to be associated with reduced
variation, although the difference was not significant. The 11
laboratories that did any duplication (duplicate blood samples,
duplicate measurements, or both) had a significantly lower SD
than did the 17 laboratories that did not. Use of an enzymatic
method to measure glucose tended to be associated with higher
refCV and SD of GI than the other analytic methods, although the
differences were not statistically significant (Table 4).
252S
WOLEVER ET AL
TABLE 3
Effect of test meal variables on outcomes1
Reference food
Glucose (n 24)
White bread (n 4)
Number of reference tests per subject
1 (n 2)
2 (n 8)
3 (n 18)
Drink type
Not specified (n 2)
Water only (n 20)
Tea or coffee allowed (n 6)
Reference AUC
Reference CV
Mean GI
SD of GI
DV
mmol min/L
213 12
230 8
22.0 1.2
26.2 5.0
58.5 1.6
62.9 5.6
22.1 1.0
26.1 6.8
1
2
265 79
199 21
217 10
22.3 3.3
22.6 1.3
65.9 3.6
59.3 3.5
58.3 1.8
23.3 1.4
24.4 2.9
21.8 1.5
215 7
210 12
232 26
21.4 3.6
23.6 1.6
19.7 1.8
55.1 2.4
54.4 1.7
51.0 2.7
20.7 0.1
22.4 1.4
17.0 1.4
1
0
2
1
All values are x SEM. The number of laboratories is indicated by n. Shown is the incremental area under the curve (AUC) for the reference food (glucose
or white bread); values for white bread were adjusted by dividing by 0.71. Reference CV is the CV (100SD/x ) of the reference AUC values for each subject.
DV is the value of the dummy variable assigned to the method variable for step-wise multiple regression analysis. GI, glycemic index.
values (Table 5). The length of the fasting time did not appear to have
any significant effect.
By univariate regression analysis, the mean GI value of the
laboratories was significantly related to 2 factors: laboratory
mean refCV (r 0.556, P 0.003; Figure 5A) and the type of
restriction placed on exercise before the test (exercise number: 0
no restriction, 1 no activity at all, 2 no unusual activity;
r 0.495, P 0.010). By multiple regression analysis, refCV
(P 0.006) and exercise number (P 0.017) together explained
46% of the variation in mean GI (ie, the coefficient of determination: r2 0.463, r 0.681, P 0.001). However, the combination of refCV (P 0.001) and the restriction placed on
TABLE 4
Effect of blood sampling and glucose measurement methods on outcomes1
Duplicate fasting blood sample
No (n 24)
Yes (n 4)
Duplicate measurement of glucose
None (n 19)
Fasting only (n 2)
All blood samples (n 6)
Any duplication
No (n 17)
Yes (n 11)
Glucose analysis method2
Enzymatic (n 9)
Hemocue (n 8)
Glucometer (n 6)
YSI (n 5)
1
Reference AUC
Reference CV
Mean GI
SD of GI
DV
mmol min/L
214 11
220 15
23.4 1.4
18.1 0.9
54.5 1.5
49.1 1.3
22.3 1.1a
14.1 0.7b
214 12
213 21
212 27
23.3 1.5
26.5 6.3
19.5 2.4
54.6 1.9
54.6 1.2
51.7 2.3
21.9 1.5
22.1 6.7
17.8 1.2
214 13
217 15
23.9 1.6
20.6 1.8
55.2 2.0
51.5 1.4
23.4 1.3a
17.5 1.4b
0
1
209 21
220 18
242 18
185 18
24.9 2.7
21.3 2.3
22.9 2.6
20.3 1.4
55.1 2.6
52.5 1.9
51.8 4.3
55.5 2.5
24.6 2.1
20.8 2.0
18.6 2.4
18.3 1.4
1
2
3
1, 3
The number of laboratories is indicated by n. Shown is the incremental area under the curve (AUC) for the reference food (glucose or white bread); values
for white bread were adjusted by dividing by 0.71. Reference CV is the CV (100SD/x ) of the reference AUC values for each subject. DV is the value of the
dummy variable assigned to the method variable for step-wise multiple regression analysis. GI, glycemic index. Means not sharing the same superscript letter
are significantly different, P 0.05.
2
Enzymatic tests included Analox GM9D Glucose Direct analyser (Waltham, MA) (n 1). Hemocue is Hemocue 201 analyzer, Hemocue AB
(Angelholm, Sweden). Glucometers used included Glucotrend (Roche Diagnostics, Basel, Switzerland) (n 1), Lifescan Surestep (Milpitas, CA) (n 1),
Ascensia (Bayer Diagnostics, Tarrytown, NY) (n 2), and Medisense (Abbott Laboratories, Abbott Park, IL) (n 1). One laboratory, which measured fasting
glucose by meter (type not specified) and postprandial glucose by using YSI, was placed into the Glucometer category. YSI is Model 2300 STAT glucose
analyzer (YSI Inc, Yellow Springs, OH). The dummy variable used for YSI was 1 for correlations with mean GI and 3 for correlations with SD of GI.
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
There was wide variation in the restrictions placed on the subjects diets and activities before the test in different laboratories.
Allowing the subjects to do usual, but not unusual, physical activities (n 5 laboratories) for 24 h before the test was associated with
significantly lower mean GI and a tendency toward reduced variation than that reported by the 10 laboratories that did not place any
restrictions on the subjects activities before the test. The results for
the 13 laboratories that did not allow any vigorous physical activity
whatsoever were intermediate (Table 5). Not allowing subjects to
consume alcoholic beverages for 24 h before the test and restricting
the type of dinner consumed or providing a standardized dinner were
associated with nonsignificant reductions in the mean and SD of GI
253S
GLYCEMIC INDEX INTERLABORATORY STUDY
TABLE 5
Effect of subject preparation variables on outcomes1
Reference AUC
Reference CV
Mean GI
SD of GI
DV
mmol min/L
229 16
185 23
216 15
24.2 2.3
20.5 2.3
22.2 1.8
58.5 2.2a
50.1 1.2b
51.4 2.0a,b
26.0 2.0
19.4 1.9
21.4 1.8
0
2
1
217 13
208 18
219 16
21.2 2.7
20.4 2.2
24.5 1.7
60.0 3.0
53.6 2.1
50.5 1.5
22.5 0.9
22.6 1.8
18.0 1.6
0
1
2
215 9
214 19
217 28
24.5 2.3
21.9 1.5
20.1 3.1
55.8 2.6
52.4 1.7
52.3 3.4
24.2 1.9
19.2 1.3
18.9 2.8
0
1
2
208 15
229 5
23.6 1.4
20.9 2.4
54.1 1.9
53.1 2.0
21.7 1.3
20.0 2.2
0
1
Vigorous activity
No restriction (n 10)
No unusual (n 5)
None at all (n 13)
Alcohol consumption3
Not specified (n 5)
None for 12 h (n 9)
None for 24 h (n 14)
Dinner the night before4
No restriction (n 11)
Restrictions (n 12)
Meal provided (n 5)
Length of fasting5
Fixed time (n 18)
None or range (n 10)
alcohol (P 0.006; 0 none, 1 none for 12 h, 2 none for
24 h) explained more of the variation in mean GI (r2 0.509,
r 0.716, P 0.001; Figure 5B), and, in this model, the effect
of exercise was not significant.
By univariate analysis, the SD of the GI in the different laboratories was significantly related to refCV (r 0.718, P
0.0001; Figure 5C), whether any duplication was performed (0
no, 1 yes; r 0.509, P 0.008), the method used for glucose
analysis (1 enzymatic, 2 Hemocue, 3 glucometer or
Yellow Springs Instruments glucose analyzer; r 0.494, P
0.010), and exercise restrictions (r 0.421, P 0.032). The
correlations between the SD and the restrictions placed on dinner
the night before (0 none, 1 restricted, 2 meal provided; r
0.386) and the type of drink allowed with the test meal (0
water only, 1 not specified, 2 coffee or tea; r 0.374)
were not statistically significant (P 0.051 and P 0.060,
respectively). By multiple linear regression analysis, refCV (P
0.001), method of glucose analysis (P 0.001), duplication (P
0.007), and restrictions on dinner (P 0.013) had significant
independent correlations with SD and together explained 81% of
the variation of SD of GI as follows: SD 0.45 refCV 3.0
method 3.6 duplication 2.2 dinner 20.5 (r 0.901,
P 0.001; Figure 5D).
DISCUSSION
The results of the present study showed that an important
source of variation in reported GI values is the way in which
different laboratories calculate the AUC and handle outlying
values. These issues will have to be addressed for regulatory
purposes. When centrally calculated GI values were considered,
the reliability of the GI method reported here was similar to that
in a previous study (32) in which the average between-laboratory
SD of GI values was 9. However, in the present study, we were
also able to see whether the characteristics of the subjects studied
or subtle variations in the methods used were associated with the
accuracy (reflected by the mean value) and precision (reflected
by the SD) of the GI results obtained by different laboratories.
Consistent with previous knowledge (3739), the glycemic
responses (ie, AUCs) of individual subjects were associated with
ethnicity and BMI. However, ethnicity, sex, age, and BMI were
not related to the within-individual variation in glycemic responses (ie, refCV) nor, most importantly, to GI values in the
individual subjects. This is consistent with previous studies suggesting that, when measured by using appropriate methods, GI is
the same in different subjects (31, 32) and therefore is a property
of the food and not of the subject in whom it is measured. The
implications of this include not only that GI can be measured
validly in most subjects but also that the results apply to most of
the healthy population.
The distribution of GI values in individual subjects is skewed
to higher values because that is a mathematical property of the
ratio of 2 independently variable measures (40). Repeating AUC
measurements can reduce skewness, which is most costeffectively achieved by repeating the reference food (32, 41).
Nevertheless, very high individual values still occur, and they
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
1
The number of laboratories is indicated by n. Shown is the incremental area under the curve (AUC) for the reference food (glucose or white bread); values
for white bread were adjusted by dividing by 0.71. Reference CV is the CV (100SD/x ) of the reference AUC values for each subject. DV is the value of the
dummy variable assigned to the method variable for step-wise multiple regression analysis. GI, glycemic index. Means not sharing the same superscript letter
are significantly different, P 0.05.
2
No restriction includes laboratories stating there was no restriction (n 6) and laboratories not specifying (n 4). None at all includes laboratories that
did not allow subjects to undertake any vigorous activity for 3 d (n 1), 24 h (n 8), 18 h (n 1), or 12 h (n 3) before the test.
3
24 h includes laboratories that advised subjects to consume no alcohol for 24 h (n 12) or 48 h (n 1) and 1 laboratory that excluded subjects who
ever used alcohol.
4
Restrictions includes laboratories allowing subjects to self-select the dinner but advising them to always have the same dinner (n 4), to avoid high-fiber
foods (n 3), to avoid legumes (n 2), to have a high-carbohydrate, low-fat meal (n 2), and to have a high-carbohydrate, high-GI meal (n 1). The types
of meals provided to subjects included solid foods (n 3), liquid test meals (n 1), and white bread and water (n 1).
5
Fixed time includes laboratories that advised subjects to fast for 8 h (n 1), 10 h (n 9), or 12 h (n 8). None or range includes laboratories that did
not specify the length of fasting time (n 3) or advised subjects to fast for 10 12 h (n 6) or 10 14 h (n 1).
254S
WOLEVER ET AL
increase the resulting mean and SD. Thus, it has been recommended that outliers should be excluded (31). Values 2 SDs
above the mean are often considered to be outliers, a cutoff that
excludes 2.5% of normally distributed values. Because GI values
are not normally distributed, a cutoff of 2 SDs may not be considered conservative enough if it results in 2.5% of the values
being excluded. However, our results show that, despite a
skewed distribution, only 2.2% of individual values were 2
SDs above the mean (95% CI: 1.33.4%). Thus, 2 SDs above
the mean appears to be an appropriate definition of GI outliers.
Only 2 (0.3%) values were 2 SDs below the mean, and, because
GI values are skewed to the right, we did not consider it appropriate or necessary to exclude these values.
Within-individual variation in glycemic responses (laboratory
mean refCV) was positively related to the mean and the SD of GI
values. The implication of this is that a high refCV leads to bias
and imprecision of the resulting GI values. Previous work suggests that refCV is affected by the blood sampling schedule,
method of calculating AUC (42), capillary versus venous blood
sampling (32, 41), and the restrictions placed on the subjects diet
and activity the day before testing (43). Here, however, the only
factor significantly related to refCV was that subjects with a low
average AUC tended to have a high refCV. This could be because
the proportion of total variation due to analytic variation becomes
larger as the AUC becomes smaller (44). Overweight subjects or
those with a family history of diabetes are sometimes excluded
from GI testing, presumably to reduce variation. Ironically, however, these exclusion criteria would have the effect of biasing the
resulting GI values toward being too high and making them
imprecise, because they would select for subjects with a low
AUC and, hence, a high refCV. The present results suggest that
mean GI is not correlated with refCV when mean refCV is 28%
(Figure 5A), and the SD of GI is not correlated with refCV when
mean refCV is 26% (Figure 5C).
The only factors related to mean GI, other than refCV, were
that restrictions on exercise and alcohol consumption before the
test were associated with lower mean GI. This unexpected result
is hard to explain. Asking subjects to avoid alcohol and exercise
doesnt guarantee that they will avoid them, and giving no advice
doesnt mean that the subjects will be exposed to them. Prior
alcohol consumption and physical activity may reduce glycemic
responses by reducing hepatic glucose output (45, 46) and improving insulin sensitivity (47 49), respectively. However, to
affect GI, the glycemic response elicited by the reference food
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
FIGURE 5. Determinants of variation in mean and SD of glycemic index (GI) values from the 26 laboratories with repeated reference tests. A: univariate
regression of mean GI on reference coefficient of variation (refCV). B: multiple regression of mean GI on refCV and restrictions on ethanol intake (EtOH). C:
univariate relation of SD of GI on refCV. D: multiple regression of SD of GI on refCV, method of glucose analysis (Mth), duplication (Dup), and nature of the
dinner the night before (Din).
GLYCEMIC INDEX INTERLABORATORY STUDY
SUMMARY OF RECOMMENDATIONS
Factors affecting the accuracy of GI
1) Calculating AUC: errors are common (50% of laboratories), and standardization is required.
2) Outliers: exclude values 2 SDs from the mean (within
laboratories).
3) Within-individual variability of AUC: mean refCV for the
subject group should be 30%.
Factors affecting the precision of GI
4) Glucose analysis: the use of a precise analytic method,
duplicating blood samples, or duplicating glucose analyses may
be beneficial; specific recommendations may depend on the analytic method used.
5) Subject preparation: moderate restrictions (eg, asking subjects to have a normal meal the night before and to avoid unusual
exercise) may be beneficial, but expensive or rigorous restrictions (eg, providing subjects with a standardized meal the night
before and prohibiting any physical activity before the test) may
have little or no additional effect.
Factors not necessary to control
6) Subject characteristics: no need to restrict the age, sex, BMI,
or ethnicity of the subjects.
7) Test meal: there may be no need to avoid coffee or tea as the
drink with the test meal.
CONCLUSIONS
The between-laboratory SD of GI values is 9 with no significant difference in mean GI between laboratories. Standardized data analysis and low within-subject variation (refCV
30%) are required for accuracy. The results suggest that common
misconceptions exist about which factors do and do not need to
be controlled to improve precision. Controlled studies and costbenefit analyses are needed to optimize GI methodology.
The contributions of the authors were as follows. TMSW: had full access
to all of the data in the study and takes responsibility for the integrity of the
data and the accuracy of the data analysis. The following letters identify the
types of contributions and are listed for each author. A: conception and design
of overall study; B: drafting and circulation of protocol, provision of central
foods, central data analysis; C: critical review of protocol (at each center;
design of procedures, acquisition of data, and calculation of results); D:
Drafting and revision of the manuscript; E: critical revision of the manuscript
for important intellectual content; F: obtained funding. TMS Wolever: A, B,
C, D, F; JC Brand-Miller: A, C, E, F; J Abernethy: C, E, F; A Astrup: C, E,
F; F Atkinson: C, E; M Axelsen: C, E, F; I Bjrk: C, E, F; F Brighenti: C, E,
F; R Brown: C, E; A Brynes: C, E; MC Casiraghi: C, E, F; M Cazaubiel: C,
E, F; L Dahlqvist: C, E; E Delport: C, E, F; GS Denyer: C, E; D Erba: C, E;
G Frost: C, E, F; Y Granfeldt: C, E; S Hampton: C, E, F; VA Hart: C,E; K
Hatnen: C, E; CJ Henry: C, E, F; S Hertzler: C, E, F; S Hull: C, E; J Jerling:
C, E, F; KL Johnston: C, E, F: H Lightowler: C, E; N Mann: C,E,F; L Morgan:
C, E, F; L Panlasigui: C, E, F; C Pelkman: C, E, F; T Perry: C, E, F; AFH
Pfeiffer: C, E, F; M Pieters: C, E; DD Ramdath: C, E, F; RT Ramsingh: C, E;
SD Robert: C, E, F; C Robinson: C,E; E Sarkkinen: C, E, F; F Scazzina: C,
E; DCD Sison: C, E; B Sloth: C, E; J Staniforth: C, E, F; N Tapola: C, E; L
Valsta: C, E, F; I Verkooijen: C, E; MO Weickert: C, E; A Weseler: C, E, F;
P Wilke: C, E; J Zhang: C, E, F.
Author statements of conflicts of interest are as follows. TMS Wolever: I
am president and part-owner of Glycemic Index Laboratories Inc, a contract
research organization and president and part-owner of Glycaemic Index
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
would have to be affected to a different extent than that after the
test food. Most laboratories used glucose as the reference food.
The cheese puffs contained more protein and fat than the glucose
did, and both test foods contained more dietary fiber than the
glucose did. The extent to which protein and fat reduce glycemic
responses may depend on subjects fasting plasma insulin, waist
circumference, fiber intake (50, 51), insulin sensitivity (52), and
possibly fat intake (53). It is not known whether the effects of
alcohol and exercise on acute glycemic responses interact with
those of other dietary factors.
We expected methodologic variables to influence the withinlaboratory SD of GI values; however, the nature of some of the
associations found was unexpected. In previous studies, the use
of 2 or 3 reference tests resulted in a lower SD than the use of only
1 (31, 41). In the present study, we could find no evidence to
justify doing 3 rather than 2 tests, because the difference was
small and not significant. Most laboratories allowed the subjects
to drink only water with the test meals, presumably to reduce
confounding factors. Unexpectedly, however, even though caffeine acutely increases glycemic responses (54), allowing drinks
of coffee and tea tended to be associated with a lower SD of GI
than drinking only water (NS; Table 3).
Taking 2 fasting blood samples, doing duplicate measurements of glucose, and using the YSI or glucometer to measure
glucose compared with the other methods used were associated
with a lower intralaboratory SD of GI. These results differ from
those of recent studies that compared some of these factors under
more controlled conditions. In a head-to-head comparison of
glucose analytic methods, GI values calculated from glucose
concentrations measured by YSI were more precise than those
measured in the same blood samples by using the One Touch
Ultra glucometer (55). However, the precision of different glucose meters varies (56), and we did not measure the precision of
the glucose analysis methods used in each laboratory. Recently,
it was shown that analyzing glucose 2 times in a single fasting
sample reduced the SD of GI values more than did using the
average of 2 different fasting samples (57). This was suggested
to be due to the fact that, in that study, the variability of the
glucose analytic method (CV 2%) was less than the minuteto-minute variation in fasting glucose (CV3%) (57); with a less
precise analytic method, it may be advantageous to take 2 fasting
blood samples.
Our results show that restricting the type of dinner the subjects
consumed the night before the test or providing a standard meal
was associated with significantly lower SD of GI values. This is
presumably because the nature of the meal consumed the night
before can carry over to influence the glycemic response the next
morning (58, 59). Providing a standardized meal to subjects
increases the cost of doing GI testing; our results suggested that
simply advising subjects to avoid certain types of foods is almost
as good and may be more cost-effective.
The results of this study should not be used to define the
required methods for GI testing for several reasons. Associations
do not prove causality; thus, our results should be used to develop
hypotheses for further testing under controlled conditions. The
costs versus benefits need to be considered. For example, the
same reduction in the margin of error achieved by providing all
subjects with a standard meal the night before every test may be
able to be achieved more economically by adding 1 or 2 more
subjects. Also, it may not be necessary to do all of the things
associated with reduced SD to obtain satisfactory results.
255S
256S
WOLEVER ET AL
REFERENCES
1. Salmeron J, Manson JE, Stampfer MJ, Colditz GA, Wing AL, Willett
WC. Dietary fiber, glycemic load and risk of non-insulin-dependent
diabetes mellitus in women. JAMA 1997;277:4727.
2. Salmeron J, Ascherio A, Rimm EB, et al. Dietary fiber, glycemic load,
and risk of NIDDM in men. Diabetes Care 1997;20:54550.
3. Liu S, Willett WC, Stampfer MJ, et al. A prospective study of dietary
glycemic load, carbohydrate intake and risk of coronary heart disease in
US women. Am J Clin Nutr 2000;71:1455 61.
4. Frost G, Leeds A, Dor CJ, Madeiros S, Brading S, Dornhorst A. Glycaemic index as a determinant of serum HDL-cholesterol concentration.
Lancet 1999;353:1045 8.
5. McKeown NM, Meigs JB, Liu S, Saltzman E, Wilson PWF, Jacques PF.
Carbohydrate nutrition, insulin resistance, and the prevalence of the
metabolic syndrome in the Framingham Offspring cohort. Diabetes Care
2004;27:538 46.
6. Liu S, Manson JE, Buring JE, Stampfer MJ, Willett WC, Rikder PM.
Relationship between a diet with a high glycemic load and plasma concentrations of high-sensitivity C-reactive protein in middle-aged
women. Am J Clin Nutr 2002;75:492 8.
7. Augustin LS, Dal Maso L, La Vecchia C, et al. Dietary glycemic index
and glycemic load, and breast cancer risk: a case-control study. Ann
Oncol 2001;12:1533 8.
8. Augustin LSA, Polesel J, Bosetti C, et al. Dietary glycemic index, glycemic load and ovarian cancer risk: a case-control study in Italy. Ann
Oncol 2003;14:78 84.
9. Augustin LSA, Gallus S, Bosetti C, et al. Glycemic index and glycemic
load in endometrial cancer. Int J Cancer 2003;105:404 7.
10. Augustin LSA, Gallus S, Franceschi S, et al. Glycemic index and load
and risk of upper aero-digestive tract neoplasms (Italy). Cancer Causes
Control 2004;14:657 62.
11. Augustin LSA, Gallus S, Negri E, La Vecchia C. Glycemic index, glycemic load and risk of gastric cancer. Ann Oncol 2004;15:581 4.
12. Augustin LSA, Galeone C, Dal Maso L, et al. Glycemic index, glycemic
load and risk of prostate cancer. Int J Cancer 2004;112:446 50.
13. Brand-Miller J, Hayne S, Petocz P, Colagiuri S. Low-glycemic index
diets in the management of diabetes: a meta-analysis of randomized
controlled trials. Diabetes Care 2003;26:22617.
14. Frost G, Leeds A, Trew G, Margara R, Dornhorst A. Insulin sensitivity
in women at risk of coronary heart disease and the effect of a low
glycemic diet. Metabolism 1998;47:124551.
15. Rizkalla SW, Taghrid L, Laromiguiere M, et al. Improved plasma glucose control, whole-body glucose utilization, and lipid profile on a lowglycemic index diet in type 2 diabetic men: a randomized trial. Diabetes
Care 2004;27:1866 72.
16. Wolever TMS, Mehling C. High-carbohydrate/low-glycaemic index dietary advice improves glucose disposition index in subjects with impaired glucose tolerance. Br J Nutr 2002;87:477 87.
17. Juntunen KS, Laaksonen DE, Poutanen KS, Niskanen LK, Mykkanen
HM. High-fiber rye bread and insulin secretion and sensitivity in healthy
postmenopausal women. Am J Clin Nutr 2003;77:38591.
18. Warren JM, Henry CJK, Simonite V. Low glycemic index breakfasts and
reduced food intake in preadolescent children. Pediatrics [serial online]
2003;112:e414. Internet: http://www.pediatrics.org/cgi/content/full/
112/5/e414 (accessed 16 February 2007).
19. Slabber M, Barnard HC, Kuyl JM, Dannhauser A, Schall R. Effects of
low-insulin-response, energy-restricted diet on weight loss and plasma
insulin concentrations in hyperinsulinemic obese females. Am J Clin
Nutr 1994;60:48 53.
20. Ebbeling CB, Leidig MM, Sinclair KB, Hangen JP, Ludwig DS. A
reduced-glycemic load diet in the treatment of adolescent obesity. Arch
Pediatr Adolesc Med 2003;157:7739.
21. McMillan-Price J, Petocz P, Atkinson F, et al. Comparison of 4 diets of
varying glycemic load on weight loss and cardiovascular risk reduction
in overweight and obese young adults. Arch Intern Med 2006;166:1466
75.
22. Kaplan RJ, Greenwood CE, Winocur G, Wolever TMS. Cognitive performance is associated with glucose regulation in healthy elderly persons
and can be enhanced with glucose and dietary carbohydrates. Am J Clin
Nutr 2000;72:82536.
23. Benton D, Ruffin MP, Lassel T, et al. The delivery rate of dietary
carbohydrates affects cognitive performance in both rats and humans.
Psychopharmacol 2003;166:86 90.
24. Kelly S, Frost G, Whittaker V, Summerbell C. Low glyacemic index
diets for coronary heart disease. Cochrane Database Syst Rev 2004;4:
CD004467.
25. Nutrition Subcommittee of the Diabetes Care Advisory Committee of
Diabetes UK. The implementation of nutritional advice for people with
diabetes. Diabetic Med 2003;20:786 807.
26. Wolever TMS, Gourgeon R, Freeze C, Field C, Thongthai K, Canadian
Diabetes Association Clinical Practice Guidelines Expert Committee.
Canadian Diabetes Association 2003 clinical practice guidelines for the
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
Testing Inc, a corporation that provides services related to the measurement
of the glycemic index of foods. I received grant and research support from
Cargill Inc and ILSI Europe, was a consultant for the US Potato Board, and
received honoraria for consulting and speaking from the Dutch Sugar Bureau
and Mars Inc. I am co-author of a range of popular books on the glycemic
index under the general title of The Glucose Revolution: Authoritative Guide
to the Glycemic Index, published by Marlowe & Co, NY. I am the author of
a scientific book titled The Glycaemic Index: A Physiologic Classification
of Dietary Carbohydrate, published by CABI, UK. Jennie C Brand-Miller
serves on the board of directors of Glycemic Index Limited, a not-for-profit
company that administers the Glycemic Index Symbol food labeling program
in Australia (www.gisymbol.com.au). She is also a director of a not-forprofit glycemic index testing service at the University of Sydney (www.
glycemicindex.com). She is a co-author on a series of books under the general
title The New Glucose Revolution (published by Marlowe and Co in North
America), which explains the theory and practice of the glycemic index to the
lay public. John Abernethy is president of AMK Research, Inc, a research
company that performs GI testing. Arne Astrup is receiving research funding
to dietary intervention studies from 100 food producers and companies and
has received speakers honoraria (Danish Meat Council, Arla Foods, Danish
Dairy Board, and Unilever) and fees for participation in advisory boards (Arla
Nutrition Advisory Board, European Almond Advisory Board, Communications and Scientific Advisory Board of the Global Dairy Platform, Proctor
& Gamble, Novartis, and Unilever) and is a medical advisor for Weight
Watcher Denmark. Furio Brighenti received research founding and consultancy fees from Barilla R&G F.lli. SpA through ParmaTecninnova SrL, a
company partly owned by the University of Parma, and at the time of the
study was a member of the following scientific boards: Beneo (a brand of
Orafti group, Belgium) and Soremartec (a company owned by Ferrero SpA).
Elizabeth Delport is one of the executive members of the GI Foundation of
SA, a contract research organization, and is a co-author on popular books on
GI. Shelagh Hampton and Linda Morgan are members of a university team
that conducts glycemic index testing for Surrey University. Valerie Hart is
employed by Reading Scientific Services, Ltd. C Jeya Henry is a member of
a university team that conducts glycemic index testing for Oxford Brookes
University. Sarah Hull is employed by Leatherhead Food International. Kelly
L Johnston was employed by Leatherhead Food International at the time of
the study. Helen Lightowler is a member of a university team that conducts
glycemic index testing for Oxford Brookes University. Christine Pelkman
has received research grants from General Mills and McNeil Nutritionals, is
a member of the International Pasta Organization Scientific Advisory Board,
and was a scientific consultant for a Readers Digest book about blood sugar.
Tracy Perry manages a GI consultancy for determination of the GI of commercially available foods Essi Sarkkinen is employed by FoodFiles Ltd.
Francesca Scazzina is recipient of a PhD bursary provided by Barilla
R&G. F.lli. SpA. Jane Staniforth is am employed by Reading Scientific
Services Ltd. Niina Tapola is employed by FoodFiles Ltd. Fiona Atkinson,
Mette Axelsen, Inger Bjrck, Rachel Brown, Audrey Brynes, M Cristina
Casiraghi, Murielle Cazaubiel, Linda Dahlqvist, Gareth Denyer, Daniela
Erba, Gary Frost, Yvonne Granfeldt, Katja Hatnen, Steve Hertzler, Johann
Jerling, Neil Mann, Leonora Panlasigui, Andreas FH Pfeiffer, Marlien
Pieters, D Dan Ramdath, Rayna T Ramsingh, S Daniel Robert, Carol
Robinson, Dave Clark Sison, Birgitte Sloth, Liisa Valsta, Inge Verkooijen,
Martin O Weickert, Antje Weseler, Paul Wilkie, and Jian Zhang had no
conflicts of interest to declare.
GLYCEMIC INDEX INTERLABORATORY STUDY
27.
28.
29.
30.
31.
32.
33.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
prior diet and activities does not reduce within-subject variation of postprandial glycemic responses to foods. Nutr Res 2003;23:6219.
Wolever TMS, Gibbs AL, Spolar M, Hitchner EV, Heimowitz C. Equivalent glycemic load (EGL): a method for quantifying the glycemic responses elicited by low carbohydrate foods. Nutr Metab (Lond) 2006;
3:33.
Siler SQ, Neese RA, Christiansen MP, Hellerstein MK. The inhibition of
gluconeogenesis following alcohol in humans. Am J Physiol 1998;275:
E897907.
Shelmet JJ, Reichard GA, Skutches CL, Hoeldtke RD, Owen OE, Boden
G. Ethanol causes acute inhibition of carbohydrate, fat and protein oxidation and insulin resistance. J Clin Invest 1988;81:1137 45.
Mikines KJ, Sonne B, Farrell PA, Tronier B, Galbo H. Effect of physical
exercise on sensitivity and responsiveness to insulin in humans. Am J
Physiol 1988;254:E248 59.
Malkova D, Evans RD, Frayn KN, Humphreys SM, Jones PR, Hardman
AE. Prior exercise and postprandial substrate extraction across the human leg. Am J Physiol 2000;279:E1020 8.
Goulet ED, Melanon MO, Aubertin-Leheudre M, Dionne IJ. Aerobic
training improves insulin sensitivity 72120h after the last exercise
session in younger but not in older women. Eur J Appl Physiol 2005;
95:146 52.
Moghaddam E, Vogt JA, Wolever TMS. The effects of fat and protein on
glycemic responses in nondiabetic humans vary with waist circumference, fasting plasma insulin, and dietary fiber intake. J Nutr 2006;136:
2506 11.
Weickert MO, Mohlig M, Koebnick C, et al. Impact of cereal fibre on
glucose-regulating factors. Diabetologia 2005;48:234353.
Brand-Miller JC, Colagiuri S, Gan ST. Insulin sensitivity predicts glycemia after a protein load. Metabolism 2000;49:15.
Cunningham KM, Daly J, Horowitz M, Read NW. Gastrointestinal adaptation to diets of differing fat composition in human volunteers. Gut
1991;32:483 6.
Battram DS, Arthur R, Weekes A, Graham TE. The glucose intolerance
induced by caffeinated coffee ingestion is less pronounced than that due
to alkaloid caffeine in men. J Nutr 2006;136:1276 80.
Velangi A, Fernandes G, Wolever TMS. Evaluation of a glucose meter
for determining the glycemic responses of foods. Clin Chim Acta 2005;
356:191 8.
Engel L, Delaney C, Cohen M. Blood glucose meters: an independent
head-to-head comparison. Pract Diabetes Int 1998;15:15 8.
Wolever TMS, Ip B, Moghaddam E. Measuring glycaemic responses:
duplicate fasting samples or duplicate measures of one fasting sample?
Br J Nutr 2006;96:799 802.
Robertson MD, Henderson RA, Vist GE, Rumsey RDE. Extended effects of evening meal carbohydrate-to-fat ratio on fasting and postprandial substrate metabolism. Am J Clin Nutr 2002;75:50510.
stman E, Presten T, Bjrk I. Effects of GI and
Nilsson A, Granfeldt Y, O
content of indigestible carbohydrates of cereal-based evening meals on
glucose tolerance at a subsequent standardized breakfast. Eur J Clin Nutr
2006;60:10929.
Downloaded from ajcn.nutrition.org by guest on October 6, 2016
34.
prevention and management of diabetes in canada: nutrition therapy.
Can J Diabetes 2003;27(suppl 2):S2731.
Perlstein RWJ, Hines C, Milsavljevic M. Dietitians Association of Australia review paper: glycaemic index in diabetes management. Australian J Nutr Dietet 1997;54:57 63.
Diabetes and Nutrition Study Group of the European Association for the
Study of Diabetes. Nutritional recommendations for the nutritional management of patients with diabetes mellitus. Eur J Clin Nutr 2000;54:
3535.
Sheard NF, Clark NG, Brand-Miller JC, et al. Dietary carbohydrate
(amount and type) in the prevention and management of diabetes: a
statement by the American Diabetes Association. Diabetes Care 2004;
27:2266 71.
Food and Agriculture Organization of the United Nations. FAO Food
and Nutrition Paper 66. Carbohydrates in human nutrition. Report of an
FAO/WHO expert consultation on carbohydrates, April 14-18, 1997,
Rome, Italy. Rome, Italy: FAO, 1998.
Brouns F, Bjorck I, Frayn KN, et al. Glycaemic index methodology. Nutr
Res Rev 2005;18:14571.
Wolever TMS, Vorster HH, Bjrk I, et al. Determination of the glycaemic index of foods: interlaboratory study. Eur J Clin Nutr 2003;57:475
82.
Deurenberg P, Deurenberg-Yap M. Validity of body composition methods across ethnic population groups. Acta Diabet 2003;40:S246 9.
Bland JM, Altman DG. Statistical methods for assessing agreement
between two methods of clinical measurement. Lancet 1986;i:30710.
Cody RP, Smith JK. Applied statistics and the SAS programming
language, 4th ed. Upper Saddle River, NJ: Prentice Hall, 1997.
Snedecor GW, Cochran WG. Statistical methods, 7th ed. Ames, IA:
Iowa State University Press, 1980.
Anand SS, Yusuf S, VuksanV, et al. Differences in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada:
the Study of Health Assessment and Risk in Ethnic groups (SHARE).
Lancet 2000;365:279 84.
Retnakaran R, Hanley AJ, Connelly PW, Sermer M, Zinman B. Ethnicity
modifies the effect of obesity on insulin resistance in pregnancy: a
comparison of Asian, South Asian, and Caucasian women J Clin Endocrinol Metab 2006;91:937.
Kahn SE, Prigeon RL, Schwartz RS, et al. Obesity, body fat distribution,
insulin sensitivity and Islet beta-cell function as explanations for metabolic diversity. J Nutr 2001;131:354S 60S.
Wolever TMS, Jenkins DJA, Jenkins AL, Josse RG. The glycemic index:
methodology and clinical implications. Am J Clin Nutr 1991;54:846
54.
Hatnen KA, Simila ME, Virtamo JR, et al. Methodologic considerations in the measurement of glycemic index: glycemic response to rye
bread, oatmeal porridge, and mashed potato. Am J Clin Nutr 2006;84:
1055 61.
Wolever TMS. Effect of blood sampling schedule and method calculating the area under the curve on validity and precision of glycaemic index
values. Br J Nutr 2004;91:295300.
Campbell JE, Glowczewski T, Wolever TMS. Controlling subjects
257S
Anda mungkin juga menyukai
- Glycaemic Index MethodologyDokumen27 halamanGlycaemic Index MethodologyGuillermo Martinez GarciaBelum ada peringkat
- Measuring The Glycemic Index of Foods: Interlaboratory StudyDokumen11 halamanMeasuring The Glycemic Index of Foods: Interlaboratory StudyGuillermo Martinez GarciaBelum ada peringkat
- The Lancet PURE 10 PDFDokumen13 halamanThe Lancet PURE 10 PDFFabrício LeãoBelum ada peringkat
- DASH and Mediterranean-Type Dietary Patterns To Maintain Cognitive HealthDokumen17 halamanDASH and Mediterranean-Type Dietary Patterns To Maintain Cognitive HealthGuillermo Martinez GarciaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Obesity and Overweight 3Dokumen65 halamanObesity and Overweight 3Productive MarsBelum ada peringkat
- Comparing Strawberry Jams Made with Stevia, Sugar and AspartameDokumen32 halamanComparing Strawberry Jams Made with Stevia, Sugar and AspartameJolly Dianne Ong100% (1)
- Three Day Water Fast and Its BenefitsDokumen11 halamanThree Day Water Fast and Its Benefitsbharath_mv7-1Belum ada peringkat
- Platepledge The Impact of NutritionDokumen4 halamanPlatepledge The Impact of Nutritiondhriti1996singhBelum ada peringkat
- Three Day Food Intake RecordDokumen12 halamanThree Day Food Intake RecordLatoya Sherice StarrBelum ada peringkat
- 10 Tips for Starting Your Wellness Journey TodayDokumen7 halaman10 Tips for Starting Your Wellness Journey TodayEzzah SobliBelum ada peringkat
- 00 The Story of MannatechDokumen25 halaman00 The Story of MannatechChristoff777Belum ada peringkat
- Listening To The News 3 - TranscriptsDokumen40 halamanListening To The News 3 - TranscriptsPhu Vo HoangBelum ada peringkat
- Body CompositionDokumen6 halamanBody CompositionRieBelum ada peringkat
- Sport England Segmenting The British Sport MarketDokumen5 halamanSport England Segmenting The British Sport MarketMojtaba Abed100% (3)
- Liquid Foods For Big CarpDokumen26 halamanLiquid Foods For Big CarpMartin SpasovskiBelum ada peringkat
- Take Care of Your Kidneys to Prevent Heart Disease and Diabetes ComplicationsDokumen2 halamanTake Care of Your Kidneys to Prevent Heart Disease and Diabetes ComplicationstimtimBelum ada peringkat
- Vazhakoombu: Kerala's famous banana variety has intrinsic health benefitsDokumen2 halamanVazhakoombu: Kerala's famous banana variety has intrinsic health benefitsKanishk KatareBelum ada peringkat
- Diabetes AwarenessDokumen12 halamanDiabetes Awarenessapi-253490911Belum ada peringkat
- Fitnessery Ultimate Ab Workouts E-BookDokumen45 halamanFitnessery Ultimate Ab Workouts E-Bookskaterchic15100% (1)
- TMD PDFDokumen45 halamanTMD PDFingbarragan87Belum ada peringkat
- PED 027 Student - S Modules 1-6Dokumen72 halamanPED 027 Student - S Modules 1-6Celina PilloraBelum ada peringkat
- Diabetes Predict Patia High Risk Report 061219Dokumen4 halamanDiabetes Predict Patia High Risk Report 061219Boo omBelum ada peringkat
- Starvation Induced Metabolic Alterations - Biochemistry For Medics - Clinical CasesDokumen6 halamanStarvation Induced Metabolic Alterations - Biochemistry For Medics - Clinical CasesDianne Faye ManabatBelum ada peringkat
- Bio4 3Dokumen10 halamanBio4 3HarmonyChuiBelum ada peringkat
- DHBenchChallenge pdf0Dokumen13 halamanDHBenchChallenge pdf0jpcmanso100% (1)
- Super Size Me Film ReportDokumen7 halamanSuper Size Me Film ReportKatharine NervaBelum ada peringkat
- SwotDokumen14 halamanSwotAlok VenuBelum ada peringkat
- Section 3Dokumen5 halamanSection 3Yo_amaranth100% (1)
- Sts SemifinalsDokumen11 halamanSts SemifinalsGerille CruzBelum ada peringkat
- Centis ReprintDokumen10 halamanCentis ReprintPragya PandeyBelum ada peringkat
- Textbook Gizi BDokumen20 halamanTextbook Gizi BShirley KawengianBelum ada peringkat
- Effect of Ultrasound Cavitation Versus Radiofrequency On Abdominal Fat Thickness in Postnatal Women 7939 - 3Dokumen12 halamanEffect of Ultrasound Cavitation Versus Radiofrequency On Abdominal Fat Thickness in Postnatal Women 7939 - 3carolina arendBelum ada peringkat
- Marching Fundamentals Handbook - 2Dokumen37 halamanMarching Fundamentals Handbook - 2Kevin ZhangBelum ada peringkat
- The 5 Fundamental of Fat LossDokumen16 halamanThe 5 Fundamental of Fat LossAndrés Jimenez100% (2)