Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Epidemiology NotesDokumen17 halamanEpidemiology NotesNash ShantolBelum ada peringkat
- Third Quarter Exam Mapeh Grade 10Dokumen4 halamanThird Quarter Exam Mapeh Grade 10Nhey Cawigan80% (118)
- Malaria Control ProgramDokumen17 halamanMalaria Control ProgramCaliso RichmondBelum ada peringkat
- Resep Baking Class 13.12.2020Dokumen4 halamanResep Baking Class 13.12.2020Nisa UcilBelum ada peringkat
- Karagol 2010Dokumen4 halamanKaragol 2010Nisa UcilBelum ada peringkat
- Faktor Risiko Ibu Dan Bayi Terhadap Kejadian Asfiksia Neonatorum Di Bali Penelitian Case Control PDFDokumen6 halamanFaktor Risiko Ibu Dan Bayi Terhadap Kejadian Asfiksia Neonatorum Di Bali Penelitian Case Control PDFNisa UcilBelum ada peringkat
- 66b3 PDFDokumen6 halaman66b3 PDFNisa UcilBelum ada peringkat
- Early Identification of Autism by The CHecklist For Autism in Toddlers CHATDokumen44 halamanEarly Identification of Autism by The CHecklist For Autism in Toddlers CHATNisa UcilBelum ada peringkat
- Heymann2007 PDFDokumen2 halamanHeymann2007 PDFNisa UcilBelum ada peringkat
- Correlation of Procalcitonin Level With NLR in Patient With SIRSDokumen1 halamanCorrelation of Procalcitonin Level With NLR in Patient With SIRSNisa UcilBelum ada peringkat
- Review Article: Autoimmune/Inflammatory Arthritis Associated Lymphomas: Who Is at Risk?Dokumen12 halamanReview Article: Autoimmune/Inflammatory Arthritis Associated Lymphomas: Who Is at Risk?Nisa UcilBelum ada peringkat
- Adrenal CrisisDokumen13 halamanAdrenal CrisisNisa UcilBelum ada peringkat
- An Unusual Presentation of Peutz-Jeghers Syndrome:: Case of Recurrent Jejunal IntussusceptionDokumen4 halamanAn Unusual Presentation of Peutz-Jeghers Syndrome:: Case of Recurrent Jejunal IntussusceptionNisa UcilBelum ada peringkat
- Postictal Todd's Paralysis Associated With Focal Cerebral Hypoperfusion On Magnetic Resonance Perfusion StudiesDokumen3 halamanPostictal Todd's Paralysis Associated With Focal Cerebral Hypoperfusion On Magnetic Resonance Perfusion StudiesNisa UcilBelum ada peringkat
- En V50n5a04Dokumen8 halamanEn V50n5a04Nisa UcilBelum ada peringkat
- Case Report: Peutz-Jeghers SyndromeDokumen3 halamanCase Report: Peutz-Jeghers SyndromeNisa UcilBelum ada peringkat
- 81337c Sanum Materia MedicaDokumen354 halaman81337c Sanum Materia MedicaTiago CostaBelum ada peringkat
- The Gamechanger by Bien Eli NillosDokumen2 halamanThe Gamechanger by Bien Eli NillosBien Elli NillosBelum ada peringkat
- Eye Banking BookDokumen135 halamanEye Banking BooknetrachikitsakBelum ada peringkat
- Preston Test 3Dokumen4 halamanPreston Test 3Aleksandra StasiakBelum ada peringkat
- Policy Analysis - Majlis Perbandaran SelayangDokumen10 halamanPolicy Analysis - Majlis Perbandaran SelayangSafwan SallehBelum ada peringkat
- 1 s2.0 S1473309922003450 MainDokumen9 halaman1 s2.0 S1473309922003450 Maincathylamont816Belum ada peringkat
- Blood Borne Helminths - Wucherelia BancroftiDokumen15 halamanBlood Borne Helminths - Wucherelia BancroftiCLEMENTBelum ada peringkat
- LEMONGRASS (Chapter 1-3 Final)Dokumen16 halamanLEMONGRASS (Chapter 1-3 Final)Criza May PascuaBelum ada peringkat
- Gastrointestinal Tract Infections - Dr. HagniDokumen40 halamanGastrointestinal Tract Infections - Dr. HagniDevi Chandra KBelum ada peringkat
- Lec 9 MalariaDokumen42 halamanLec 9 MalariaMye AkmaBelum ada peringkat
- Penetration of Anti Infective Agents Into.3Dokumen28 halamanPenetration of Anti Infective Agents Into.3Thawatchai NakkaratniyomBelum ada peringkat
- Antibiofilm Activity and Post Antifungal Effect of Lemongrass Oil On Clinical Candida Dubliniensis IsolateDokumen7 halamanAntibiofilm Activity and Post Antifungal Effect of Lemongrass Oil On Clinical Candida Dubliniensis Isolatezila_w2gBelum ada peringkat
- Utah State Hospital Policies and Procedures Infection ControlDokumen75 halamanUtah State Hospital Policies and Procedures Infection ControlMichael SilvaBelum ada peringkat
- Medhub CoagulaseDokumen7 halamanMedhub Coagulasemedical ChyBelum ada peringkat
- Sinusitis - University of Maryland Medical CenterDokumen17 halamanSinusitis - University of Maryland Medical CenterDwiKamaswariBelum ada peringkat
- CHN RN PediaDokumen24 halamanCHN RN Pediamarieekariee777Belum ada peringkat
- NGL - Covid-19 - ELA-Reading Lesson - WS - FPPDokumen5 halamanNGL - Covid-19 - ELA-Reading Lesson - WS - FPPAhmed ElabbacyBelum ada peringkat
- G1 Research Proposal FINALDokumen25 halamanG1 Research Proposal FINALjessrelle.gumawaBelum ada peringkat
- Joint Waiver On Covid-19 VaccinationDokumen2 halamanJoint Waiver On Covid-19 VaccinationAlexanderBelum ada peringkat
- Repair of Vaginal and Perineal Tears22Dokumen4 halamanRepair of Vaginal and Perineal Tears22Francez Anne GuanzonBelum ada peringkat
- Emerging and Reemerging InfectionDokumen1 halamanEmerging and Reemerging InfectionKurt Bryan CortezBelum ada peringkat
- Amebiasis. Aspectos Clínicos, Terapéuticos y de Diagnóstico PDFDokumen7 halamanAmebiasis. Aspectos Clínicos, Terapéuticos y de Diagnóstico PDFDina EuniseBelum ada peringkat
- Country Statement Sample For MALDokumen2 halamanCountry Statement Sample For MALtem199767% (3)
- Puesta Al Día: Neumonía Comunitaria: J. Vasco Barreto - 7/5/2022Dokumen39 halamanPuesta Al Día: Neumonía Comunitaria: J. Vasco Barreto - 7/5/2022Claudia RamírezBelum ada peringkat
- QB - L03 - Fibre To Fabric - QPDokumen3 halamanQB - L03 - Fibre To Fabric - QPPankaj SinghBelum ada peringkat
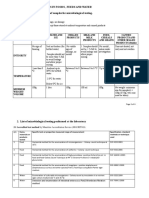
- Microbiological Tests in Foods, Feeds and Water 1. Guidelines For Submission of Samples For Microbiological TestingDokumen3 halamanMicrobiological Tests in Foods, Feeds and Water 1. Guidelines For Submission of Samples For Microbiological Testing111280Belum ada peringkat
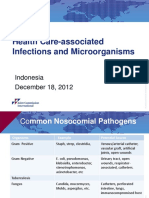
- Microbiology of HAIDokumen21 halamanMicrobiology of HAIDevi Pateubih WaosBelum ada peringkat