Anda mungkin juga menyukai
- Structural Integrity ManagementDokumen12 halamanStructural Integrity Managementonnly1964Belum ada peringkat
- TS Coating Characterization SiegmannDokumen22 halamanTS Coating Characterization Siegmannonnly1964Belum ada peringkat
- 12 Structural Integrity Management - Ersdal - PtilDokumen10 halaman12 Structural Integrity Management - Ersdal - PtilEyoma EtimBelum ada peringkat
- Structural Integrity Management: Ageing Structures Workshop April 8thDokumen10 halamanStructural Integrity Management: Ageing Structures Workshop April 8thonnly1964Belum ada peringkat
- Structural Integrity ManagementDokumen12 halamanStructural Integrity Managementonnly1964Belum ada peringkat
- Structural Integrity ManagementDokumen22 halamanStructural Integrity Managementonnly1964100% (1)
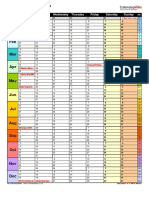
- Calendar 2017 Landscape Year at A GlanceDokumen1 halamanCalendar 2017 Landscape Year at A Glanceonnly1964Belum ada peringkat
- Specimen Grips and Test Tools PDFDokumen20 halamanSpecimen Grips and Test Tools PDFAhmed MagdyBelum ada peringkat
- Structural Integrity ManagementDokumen12 halamanStructural Integrity Managementonnly1964Belum ada peringkat
- Calendar 2017 Portrait RollingDokumen1 halamanCalendar 2017 Portrait Rollingonnly1964Belum ada peringkat
- Calendar 2017 Portrait RollingDokumen1 halamanCalendar 2017 Portrait Rollingonnly1964Belum ada peringkat
- IMoM 6BDokumen42 halamanIMoM 6BDaniel Laurence Salazar ItableBelum ada peringkat
- Structural Integrity ManagementDokumen12 halamanStructural Integrity Managementonnly1964Belum ada peringkat
- Calendar 2017 Landscape Year at A GlanceDokumen1 halamanCalendar 2017 Landscape Year at A Glanceonnly1964Belum ada peringkat
- Distributed Intelligent Systems: Cursus Sem. TypeDokumen2 halamanDistributed Intelligent Systems: Cursus Sem. Typeonnly1964Belum ada peringkat
- Calendar 2017 Landscape PDFDokumen1 halamanCalendar 2017 Landscape PDFonnly1964Belum ada peringkat
- NRES Report IllustrationDokumen2 halamanNRES Report Illustrationonnly1964Belum ada peringkat
- Calculation of The Crosshead Velocity Required To Achieve A Specified Stress Rate or An Estimated Strain RateDokumen9 halamanCalculation of The Crosshead Velocity Required To Achieve A Specified Stress Rate or An Estimated Strain Ratemp87_ing100% (1)
- 8801 Servohydraulic Fatigue Testing System: Up To 100 KNDokumen4 halaman8801 Servohydraulic Fatigue Testing System: Up To 100 KNonnly1964Belum ada peringkat
- Universal Sheet Metal Testing Machine Model 146: Maximum Strain Deep Drawing Cup TestDokumen4 halamanUniversal Sheet Metal Testing Machine Model 146: Maximum Strain Deep Drawing Cup Testonnly1964Belum ada peringkat
- Renewable Energy: Wenyi Liu, Baoping Tang, Yonghua JiangDokumen5 halamanRenewable Energy: Wenyi Liu, Baoping Tang, Yonghua Jiangonnly1964Belum ada peringkat
- MagnetizingGuide PDFDokumen50 halamanMagnetizingGuide PDFonnly1964Belum ada peringkat
- Composite Specimen Bearing Failure Reduction in Iosipescu Shear TestsDokumen7 halamanComposite Specimen Bearing Failure Reduction in Iosipescu Shear Testsonnly1964Belum ada peringkat
- Bulge/ FLC Tester Model 161: Testing Equipment For Quality ManagementDokumen4 halamanBulge/ FLC Tester Model 161: Testing Equipment For Quality Managementonnly1964Belum ada peringkat
- Calendar 2017 LandscapeDokumen1 halamanCalendar 2017 Landscapeonnly1964Belum ada peringkat
- Triaxial SampleDokumen1 halamanTriaxial Sampleonnly1964Belum ada peringkat
- Pressure VesselDokumen32 halamanPressure VesselYonjon SubhaBelum ada peringkat
- SolidWorksToAbaqus AIDokumen28 halamanSolidWorksToAbaqus AIonnly1964Belum ada peringkat
- 3d Sample EightDokumen1 halaman3d Sample Eightonnly1964Belum ada peringkat
- 3d SampleDokumen1 halaman3d Sampleonnly1964Belum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Lesson Plans Obesity Diabetes and HypertDokumen12 halamanLesson Plans Obesity Diabetes and HypertPrince Rupee GonzalesBelum ada peringkat
- Prevention of Diabetic Foot Ulcers The Bottlenecks in The PathwayDokumen3 halamanPrevention of Diabetic Foot Ulcers The Bottlenecks in The PathwayreuniBelum ada peringkat
- WC 500044213Dokumen2 halamanWC 500044213pppijkBelum ada peringkat
- Nursing Acn-IiDokumen80 halamanNursing Acn-IiMunawar100% (6)
- The Blood Sugar MiracleDokumen63 halamanThe Blood Sugar MiracleRick Swartz80% (5)
- Molecular Basis of Type 2 DiabetesDokumen22 halamanMolecular Basis of Type 2 DiabetespimpellerBelum ada peringkat
- Update On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal MedicineDokumen217 halamanUpdate On Medical Disorders in Pregnancy An Issue of Obstetrics and Gynecology Clinics The Clinics Internal Medicinemeriatmaja100% (1)
- Cardiovascular Disease: By: Bs Nutrition and Dietetics StudentsDokumen13 halamanCardiovascular Disease: By: Bs Nutrition and Dietetics StudentsMiles ViaBelum ada peringkat
- Terms/ Choices/questions Given by Other Students With The Same RecallDokumen27 halamanTerms/ Choices/questions Given by Other Students With The Same RecallchippaiqweqweBelum ada peringkat
- Effect of Chewing Tobacco On Fasting Blood Glucose LevelsDokumen3 halamanEffect of Chewing Tobacco On Fasting Blood Glucose LevelsAdvaitBelum ada peringkat
- (PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFDokumen5 halaman(PhysioEX Chapter 4 Exercise 2) PEX-04-02 - Steemit PDFshennie ante100% (1)
- The Belly Fat Diet John ChathamDokumen92 halamanThe Belly Fat Diet John ChathamGurpreet Kaur100% (3)
- Gliptins: Current Status & Future PromiseDokumen46 halamanGliptins: Current Status & Future PromiseSmit ShahBelum ada peringkat
- Diabetes For EMS ProvidersDokumen58 halamanDiabetes For EMS ProvidersPaulhotvw67100% (2)
- Calabash 19 FINALDokumen80 halamanCalabash 19 FINALJani Misterio75% (4)
- Presented By: Aprindo Donatus Consultant: Dr. Iqbal Lahmadi, SP - PDDokumen13 halamanPresented By: Aprindo Donatus Consultant: Dr. Iqbal Lahmadi, SP - PDAprindoDonatusBelum ada peringkat
- National Geographic March 2016Dokumen148 halamanNational Geographic March 2016Anonymous Azxx3Kp9Belum ada peringkat
- Prasugrel and RosuvastatinDokumen7 halamanPrasugrel and RosuvastatinMohammad Shahbaz AlamBelum ada peringkat
- Diabetes Resommendations Laboratory AnalysisDokumen120 halamanDiabetes Resommendations Laboratory AnalysisAleja Coneja BonifazBelum ada peringkat
- Materi SeminarDokumen5 halamanMateri SeminarKota KisaranBelum ada peringkat
- Exercise As Defensive Nutritional Paradigm - MSC Sem3FPP - 19-20 - NALSDokumen18 halamanExercise As Defensive Nutritional Paradigm - MSC Sem3FPP - 19-20 - NALSdrashti shahBelum ada peringkat
- Presented by DR Ashish Sharma Guided by DR Meena PatelDokumen74 halamanPresented by DR Ashish Sharma Guided by DR Meena PatelAndrew Surya Putra SccBelum ada peringkat
- The Blood Pressure Solution Ebook 022318Dokumen14 halamanThe Blood Pressure Solution Ebook 022318Rolando M Tabora100% (2)
- Concise Review: Importance of Probiotics Yogurt For Human Health ImprovementDokumen6 halamanConcise Review: Importance of Probiotics Yogurt For Human Health ImprovementIOSRjournalBelum ada peringkat
- Rising Incidence of Overweight and Obesity Among Children and Adolescents in IndiaDokumen8 halamanRising Incidence of Overweight and Obesity Among Children and Adolescents in IndiaSSR-IIJLS JournalBelum ada peringkat
- InvokanaDokumen14 halamanInvokanaalvaroBelum ada peringkat
- Case Study 1 - DMDokumen9 halamanCase Study 1 - DMapi-368453103Belum ada peringkat
- PDHPE Notes - Health Priorities in Australia 3Dokumen99 halamanPDHPE Notes - Health Priorities in Australia 3EvonneBelum ada peringkat