Anda mungkin juga menyukai
- 2006 Acute Vascular Responses To Isometric Handgrip Exercise and Effects of Training in Persons MDokumen7 halaman2006 Acute Vascular Responses To Isometric Handgrip Exercise and Effects of Training in Persons MDavid HaluliBelum ada peringkat
- Restrição Calorica e Sistema ImuneDokumen24 halamanRestrição Calorica e Sistema ImuneDavid HaluliBelum ada peringkat
- 2006 Caffeine Attenuates Early Post-Exercise HypotensionDokumen5 halaman2006 Caffeine Attenuates Early Post-Exercise HypotensionDavid HaluliBelum ada peringkat
- 2005 Resistance Exercise On Blood Pressure in OldersDokumen8 halaman2005 Resistance Exercise On Blood Pressure in OldersDavid HaluliBelum ada peringkat
- 2005 Effectiveness of Self-Measurement of Blood Pressure HEM 705CP OMRONDokumen7 halaman2005 Effectiveness of Self-Measurement of Blood Pressure HEM 705CP OMRONDavid HaluliBelum ada peringkat
- 2005 Effect of Exercise On Blood Pressure in Older PersonsDokumen7 halaman2005 Effect of Exercise On Blood Pressure in Older PersonsDavid HaluliBelum ada peringkat
- 2007 Pulmonary Rehabilitation Joint Accp Aacvpr Evidence Based Clinical Practice GuidelinesDokumen41 halaman2007 Pulmonary Rehabilitation Joint Accp Aacvpr Evidence Based Clinical Practice GuidelinesDavid HaluliBelum ada peringkat
- Writing About CreatineDokumen2 halamanWriting About CreatineDavid HaluliBelum ada peringkat
- 2005 - Fulco - Carbohydrate Supplementation Improves Time-Trial Cycle PerformanceDokumen41 halaman2005 - Fulco - Carbohydrate Supplementation Improves Time-Trial Cycle PerformanceDavid HaluliBelum ada peringkat
- 2005 Glutamine and Arginine ImmunonutrientsDokumen2 halaman2005 Glutamine and Arginine ImmunonutrientsDavid HaluliBelum ada peringkat
- Acute Interval Exercise Intensity Does Not Affect Appetite and Nutrient Preferences in Overweight and Obese MalesDokumen7 halamanAcute Interval Exercise Intensity Does Not Affect Appetite and Nutrient Preferences in Overweight and Obese MalesDavid HaluliBelum ada peringkat
- Yo-YO TrestDokumen5 halamanYo-YO TrestDavid HaluliBelum ada peringkat
- Voluntary ExerciseDokumen7 halamanVoluntary ExerciseDavid HaluliBelum ada peringkat
- Why Combine Diet and Physical ActivityDokumen10 halamanWhy Combine Diet and Physical ActivityDavid HaluliBelum ada peringkat
- 2006 L-Arginine - Ketoglutarate in Trained Adult MenDokumen10 halaman2006 L-Arginine - Ketoglutarate in Trained Adult MenDavid HaluliBelum ada peringkat
- 2006 Post-Resistance Exercise Hypotension Influence of IntensityDokumen8 halaman2006 Post-Resistance Exercise Hypotension Influence of IntensityDavid HaluliBelum ada peringkat
- 2006 Rest Interval Between Resistance Training ReviewDokumen8 halaman2006 Rest Interval Between Resistance Training ReviewDavid HaluliBelum ada peringkat
- 2006 Sarcopenia Exercise As Treatment StrategyDokumen4 halaman2006 Sarcopenia Exercise As Treatment StrategyDavid HaluliBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- HFS PHILIPPINES, INC., G.R. No. 168716 Ruben T. Del Rosario and Ium Shipmanagement As, Petitioners, Ronaldo R. Pilar, Respondent. PromulgatedDokumen8 halamanHFS PHILIPPINES, INC., G.R. No. 168716 Ruben T. Del Rosario and Ium Shipmanagement As, Petitioners, Ronaldo R. Pilar, Respondent. PromulgateddanexrainierBelum ada peringkat
- 6 Metronidazole Drug StudyDokumen4 halaman6 Metronidazole Drug Studyshadow gonzalezBelum ada peringkat
- Konversi Insulin IV-sc 2Dokumen12 halamanKonversi Insulin IV-sc 2Nurul Kamilah SadliBelum ada peringkat
- Spring Meadows Hospital VsDokumen10 halamanSpring Meadows Hospital VsManoj Kumar MBelum ada peringkat
- PERIMETRY Introduction GuideDokumen70 halamanPERIMETRY Introduction GuideDana Andreea Popescu100% (1)
- Can Oral Sex Cause Throat CancerDokumen4 halamanCan Oral Sex Cause Throat CancerjyuldipBelum ada peringkat
- Optimization of Granulation and Compression Process Variables of Atenolol Tablets Using Box Behnken DesignDokumen9 halamanOptimization of Granulation and Compression Process Variables of Atenolol Tablets Using Box Behnken DesignnkszoneBelum ada peringkat
- Intramedullary Nailing For Femur Fracture Web Version EnglishDokumen6 halamanIntramedullary Nailing For Femur Fracture Web Version EnglishCarima JatnoBelum ada peringkat
- Philosophy of OcclusionDokumen23 halamanPhilosophy of OcclusionAnil SukumaranBelum ada peringkat
- GTT Porcelain PDFDokumen21 halamanGTT Porcelain PDFYAALINY YKBelum ada peringkat
- Circulatory SystemDokumen5 halamanCirculatory SystemMissDyYournurse100% (1)
- Manual Neo 900Dokumen76 halamanManual Neo 900Bismarck Pablo Ibañez Piotti67% (3)
- MedicineDokumen17 halamanMedicineSubhashini R0% (1)
- 200 Terms & Definition From Pharmacology. WatermarkedDokumen17 halaman200 Terms & Definition From Pharmacology. Watermarkedsuresh adgaonkar100% (1)
- Top 5 Lavender Home RemediesDokumen16 halamanTop 5 Lavender Home RemediesjeslynBelum ada peringkat
- Homeostatic Effect of Laughter On Diabetic Cardiovascular Complications: The Myth Turned To FactDokumen9 halamanHomeostatic Effect of Laughter On Diabetic Cardiovascular Complications: The Myth Turned To FactNona HenBelum ada peringkat
- Orientation To Blood Bank 2Dokumen24 halamanOrientation To Blood Bank 2Darshita SharmaBelum ada peringkat
- Mix It Up and SqueezeDokumen3 halamanMix It Up and Squeezeapi-233757247100% (1)
- Sistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022Dokumen13 halamanSistem Pelaporan Dan Pembelajaran Keselamatan Pasien RS Arjaty 2022vera kusunyadewiBelum ada peringkat
- Oral Alerting ActivitiesDokumen3 halamanOral Alerting ActivitiesAnn VillablancaBelum ada peringkat
- Biggs Medicine, SurgeryDokumen19 halamanBiggs Medicine, Surgerymary20149Belum ada peringkat
- FHP & NCP - FractureDokumen14 halamanFHP & NCP - FractureFrancis AdrianBelum ada peringkat
- Human Anatomy QsDokumen31 halamanHuman Anatomy QsAzhagar Ramesh SBelum ada peringkat
- Flip Chart 06 IUDDokumen12 halamanFlip Chart 06 IUDLamyaa Ali HasanBelum ada peringkat
- Endocrine Glands The Producers of Chemical MessengersDokumen10 halamanEndocrine Glands The Producers of Chemical Messengersahmed100% (1)
- Kampa VataDokumen27 halamanKampa VataAditya Tak100% (1)
- Theraputic UltrasoundDokumen64 halamanTheraputic UltrasoundRoshni KhanBelum ada peringkat
- Antidepression ReikiDokumen6 halamanAntidepression ReikiDoc Lyman88% (8)
- Outbreak Investigation Part 1 PDFDokumen4 halamanOutbreak Investigation Part 1 PDFashythegreat93Belum ada peringkat
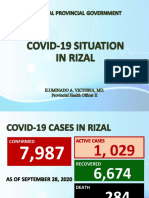
- Covid19 Situation in RizalDokumen23 halamanCovid19 Situation in RizalToni Quitalig GamezBelum ada peringkat