Anda mungkin juga menyukai
- Transcultural Health TranscriptDokumen4 halamanTranscultural Health TranscriptJane Mae JesoroBelum ada peringkat
- NCM 120 MidtermDokumen6 halamanNCM 120 MidtermArrianne NatividadBelum ada peringkat
- Chinese Culture ClueDokumen2 halamanChinese Culture ClueSr. RZBelum ada peringkat
- Health Mathew1Dokumen66 halamanHealth Mathew1averagehealerBelum ada peringkat
- Concepts and Perceptions of Health, Illness, and Disease/ Healing SystemDokumen21 halamanConcepts and Perceptions of Health, Illness, and Disease/ Healing SystemAyaz LatifBelum ada peringkat
- Special Issues in The Delivery of Transcultural Nursing CareDokumen32 halamanSpecial Issues in The Delivery of Transcultural Nursing CareMushtaq Ali100% (13)
- NCM 120 Week 6 Topic 5Dokumen83 halamanNCM 120 Week 6 Topic 5Ma. Esperanza C. Eijansantos-Reavon50% (2)
- 3e - End of Life Care-Russian PDFDokumen2 halaman3e - End of Life Care-Russian PDFtemp001bunnBelum ada peringkat
- Culture Practices, Gender and Impact On HealthDokumen31 halamanCulture Practices, Gender and Impact On HealthNatukunda Dianah100% (1)
- Cultural Perspectives in ChildbearingDokumen4 halamanCultural Perspectives in ChildbearingdulceRNBelum ada peringkat
- Cultural Awareness, Legal NSG, Delgation, Prioritization, Electrolyte, ABG AnalysisDokumen343 halamanCultural Awareness, Legal NSG, Delgation, Prioritization, Electrolyte, ABG AnalysisReeya RayamajhiBelum ada peringkat
- Cultural AssessmentDokumen2 halamanCultural AssessmentvhonBelum ada peringkat
- Culturally Competent Nursing CareDokumen22 halamanCulturally Competent Nursing CareFrancia ToledanoBelum ada peringkat
- Module 5 Health Belief, Healing Trad.Dokumen18 halamanModule 5 Health Belief, Healing Trad.samrasahluBelum ada peringkat
- Obstacles To Medical CareDokumen9 halamanObstacles To Medical CareElle MongeBelum ada peringkat
- Nursing and End-of-Life CareDokumen26 halamanNursing and End-of-Life CareShafiq Ur RahmanBelum ada peringkat
- NCM 114 Care of The Older Adult Emelie Jalandoni Tan, RN., DnsDokumen7 halamanNCM 114 Care of The Older Adult Emelie Jalandoni Tan, RN., DnsPatricia Vasquez100% (4)
- Presentation On Medical AnthropologyDokumen16 halamanPresentation On Medical AnthropologyWasima TabassumBelum ada peringkat
- Cultural Competence and Patient-Centered Care: Horblit Health Sciences LibraryDokumen21 halamanCultural Competence and Patient-Centered Care: Horblit Health Sciences LibraryKristine C.Belum ada peringkat
- Communication in Terminally Ill PatientsDokumen28 halamanCommunication in Terminally Ill PatientsHarfiyyah HmrBelum ada peringkat
- Concepts and Perception of Health, Illness &updatedDokumen17 halamanConcepts and Perception of Health, Illness &updatednabeelpatras19Belum ada peringkat
- Final Power Point 2Dokumen53 halamanFinal Power Point 2Eric RosalesBelum ada peringkat
- 5 Steps: Medical Care Decision Making For Families and Guardians. July 2013Dokumen2 halaman5 Steps: Medical Care Decision Making For Families and Guardians. July 2013Dr Jerome MellorBelum ada peringkat
- Communicating With Patients From Different Cultural BackgroundDokumen24 halamanCommunicating With Patients From Different Cultural BackgroundRiska Aprilia100% (1)
- PCARE Week3Dokumen12 halamanPCARE Week3;'SiLeNt';Belum ada peringkat
- Concepts of Health Wellness and Well BeingDokumen6 halamanConcepts of Health Wellness and Well Beinglai.creates4uBelum ada peringkat
- Funds Final BlueprintDokumen5 halamanFunds Final BlueprintAudry GuillermoBelum ada peringkat
- Mexican CultureDokumen26 halamanMexican Cultureapi-607314474Belum ada peringkat
- Mental Health Nursing II NURS 2310: Unit IV Cultural Considerations For The Psychiatric/Mental Health ClientDokumen25 halamanMental Health Nursing II NURS 2310: Unit IV Cultural Considerations For The Psychiatric/Mental Health ClientKJ BinduBelum ada peringkat
- Change Your Diet, Change Your Health: How Food Can Maintain Our Health or Cause DiseaseDari EverandChange Your Diet, Change Your Health: How Food Can Maintain Our Health or Cause DiseaseBelum ada peringkat
- Funda Basic Care and ComfortDokumen11 halamanFunda Basic Care and Comfortjericho obiceBelum ada peringkat
- Presentation - 2 End of Life CareDokumen32 halamanPresentation - 2 End of Life CareDaneshwari Sahu100% (1)
- Understanding Transcultural NursingDokumen7 halamanUnderstanding Transcultural NursingVALENZUELA DELIESA E.100% (1)
- Lesson 3 Nutritional AssessmentDokumen84 halamanLesson 3 Nutritional AssessmentJake ArizapaBelum ada peringkat
- Example File XDokumen5 halamanExample File XGabriel DATY at QuickofficeBelum ada peringkat
- Clouds and Sunshine: A Personal View of Life after a Cancer DiagnosisDari EverandClouds and Sunshine: A Personal View of Life after a Cancer DiagnosisBelum ada peringkat
- Cult Comp CareDokumen15 halamanCult Comp CareKharis Mochammad NurBelum ada peringkat
- Global Health Lectue FiveDokumen22 halamanGlobal Health Lectue FiveHassan Kafi AliBelum ada peringkat
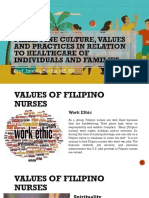
- Philippine Culture Values and Practices in Relation To Healthcare of Individuals and FamiliesDokumen22 halamanPhilippine Culture Values and Practices in Relation To Healthcare of Individuals and FamiliesKhams Tolentino0% (1)
- Culture PaperDokumen10 halamanCulture PaperJason HarrisonBelum ada peringkat
- Trans CulturalDokumen6 halamanTrans CulturalAlyssa Santos JavierBelum ada peringkat
- Overview of Mental Health NursingDokumen2 halamanOverview of Mental Health NursingderrickBelum ada peringkat
- Filipino Culture Values and Practices in Relation To Drug Administration 1 4 PDFDokumen3 halamanFilipino Culture Values and Practices in Relation To Drug Administration 1 4 PDFBianca Marithè RejanoBelum ada peringkat
- Life and DeathDokumen23 halamanLife and DeathJea Joel MendozaBelum ada peringkat
- Penyaji: Ivan Veriswan: Diambil Dari Handbook of Adolescent Medicine and Health PromotionDokumen19 halamanPenyaji: Ivan Veriswan: Diambil Dari Handbook of Adolescent Medicine and Health PromotionIvan VeriswanBelum ada peringkat
- Cultural Diversity in NursingDokumen7 halamanCultural Diversity in NursingIconMaicoBelum ada peringkat
- Fundamentals of Nursing Nclex RNDokumen71 halamanFundamentals of Nursing Nclex RNspartacuslivesBelum ada peringkat
- Health Care SystemDokumen11 halamanHealth Care SystemWasima TabassumBelum ada peringkat
- Health and IllnessDokumen20 halamanHealth and IllnessCoasfan CossyBelum ada peringkat
- MENTAL HEALTH Remdiation-PasspointDokumen3 halamanMENTAL HEALTH Remdiation-PasspointSarahjane LegaspiBelum ada peringkat
- Anorexia NervosaDokumen3 halamanAnorexia NervosaLiezle Joy Agawin GargolesBelum ada peringkat
- Fundamentals of Nursing (Nclex-Rn)Dokumen71 halamanFundamentals of Nursing (Nclex-Rn)Peter John Ruiz100% (5)
- Care Seeking BehaviourDokumen13 halamanCare Seeking BehaviourAnonymous FfZm5kOkYFBelum ada peringkat
- Palliative CareDokumen82 halamanPalliative Carejoycebrenda348Belum ada peringkat
- Approaches For Cross Cultural RelationshipsDokumen3 halamanApproaches For Cross Cultural RelationshipsMădălina OanceaBelum ada peringkat
- Recover Your Health: Simple Uncensored Health StrategiesDari EverandRecover Your Health: Simple Uncensored Health StrategiesBelum ada peringkat
- Look Hot, Live Long: The Prescription for Women Who Want to Look Their Best While Enjoying a Long and Healthy LifeDari EverandLook Hot, Live Long: The Prescription for Women Who Want to Look Their Best While Enjoying a Long and Healthy LifeBelum ada peringkat
- Clearing the Way to Health and Wellness: Reversing Chronic Conditions by Freeing the Body of Food, Environmental, and Other SensitivitiesDari EverandClearing the Way to Health and Wellness: Reversing Chronic Conditions by Freeing the Body of Food, Environmental, and Other SensitivitiesBelum ada peringkat
- Main Girders: CrossDokumen3 halamanMain Girders: Crossmn4webBelum ada peringkat
- SCM (Subway Project Report)Dokumen13 halamanSCM (Subway Project Report)Beast aBelum ada peringkat
- 300 PSI CTS (MP-1115) Operation Manual Rev1.3Dokumen18 halaman300 PSI CTS (MP-1115) Operation Manual Rev1.3Juan Manuel VizosoBelum ada peringkat
- Lecture 12Dokumen8 halamanLecture 12Mechanical ZombieBelum ada peringkat
- Shree New Price List 2016-17Dokumen13 halamanShree New Price List 2016-17ontimeBelum ada peringkat
- Curing Obesity, WorldwideDokumen6 halamanCuring Obesity, WorldwideHernán SanabriaBelum ada peringkat
- Mockery Breed Murder Birds PDFDokumen12 halamanMockery Breed Murder Birds PDFLautaro BojanichBelum ada peringkat
- JRC JFE-680 Instruct ManualDokumen86 halamanJRC JFE-680 Instruct ManualMark Dominic FedericoBelum ada peringkat
- TreesDokumen69 halamanTreesADITYA GEHLAWATBelum ada peringkat
- CheckList For Checking of Drawings-R1Dokumen4 halamanCheckList For Checking of Drawings-R1jatin kalraBelum ada peringkat
- Math COT 3Dokumen18 halamanMath COT 3Icy Mae SenadosBelum ada peringkat
- Nissan Copper LTDDokumen11 halamanNissan Copper LTDankit_shahBelum ada peringkat
- 123 09-Printable Menu VORDokumen2 halaman123 09-Printable Menu VORArmstrong TowerBelum ada peringkat
- PPT DIARHEA IN CHILDRENDokumen31 halamanPPT DIARHEA IN CHILDRENRifka AnisaBelum ada peringkat
- Passenger Lift Alert - Health and Safety AuthorityDokumen4 halamanPassenger Lift Alert - Health and Safety AuthorityReginald MaswanganyiBelum ada peringkat
- Plans PDFDokumen49 halamanPlans PDFEstevam Gomes de Azevedo85% (34)
- 5G Transport Slice Control in End-To-End 5G NetworksDokumen19 halaman5G Transport Slice Control in End-To-End 5G NetworksmorganBelum ada peringkat
- Dusta ManaDokumen16 halamanDusta ManamahaphalaBelum ada peringkat
- Catalogo GatesDokumen255 halamanCatalogo GatesBenjamin HedoneweBelum ada peringkat
- Combined Shear and TensionDokumen16 halamanCombined Shear and TensionDAN MARK OPONDABelum ada peringkat
- Tesla Coil ProjectDokumen8 halamanTesla Coil ProjectShivam singhBelum ada peringkat
- Bomba MixerDokumen2 halamanBomba MixerBinelli79Belum ada peringkat
- Niir Integrated Organic Farming Handbook PDFDokumen13 halamanNiir Integrated Organic Farming Handbook PDFNatalieBelum ada peringkat
- Worlds Apart: A Story of Three Possible Warmer WorldsDokumen1 halamanWorlds Apart: A Story of Three Possible Warmer WorldsJuan Jose SossaBelum ada peringkat
- Bulacan Agricultural State College: Lesson Plan in Science 4 Life Cycle of Humans, Animals and PlantsDokumen6 halamanBulacan Agricultural State College: Lesson Plan in Science 4 Life Cycle of Humans, Animals and PlantsHarmonica PellazarBelum ada peringkat
- Electricity NotesDokumen35 halamanElectricity Notesapi-277818647Belum ada peringkat
- BC-6000 Installation Guide V7.0 enDokumen111 halamanBC-6000 Installation Guide V7.0 enmentule88Belum ada peringkat
- FRP Handrail Fittings CatalogDokumen6 halamanFRP Handrail Fittings CatalogAl Adel MorenoBelum ada peringkat
- GP1 Q1 Week-1Dokumen18 halamanGP1 Q1 Week-1kickyknacksBelum ada peringkat
- Study The Effect of Postharvest Heat Treatment On Infestation Rate of Fruit Date Palm (Phoenix Dactylifera L.) Cultivars Grown in AlgeriaDokumen4 halamanStudy The Effect of Postharvest Heat Treatment On Infestation Rate of Fruit Date Palm (Phoenix Dactylifera L.) Cultivars Grown in AlgeriaJournal of Nutritional Science and Healthy DietBelum ada peringkat