Anda mungkin juga menyukai
- Chest Wall DisordersDokumen66 halamanChest Wall DisordersSwathi VivekBelum ada peringkat
- 9 Anaesthetic Considerations For Laparoscopic Surgery in Neonates and Infants: A Practical ReviewDokumen13 halaman9 Anaesthetic Considerations For Laparoscopic Surgery in Neonates and Infants: A Practical Reviewdiomer123Belum ada peringkat
- Obesidad y Pulmón Thorax 2008Dokumen7 halamanObesidad y Pulmón Thorax 2008Peter CabezasBelum ada peringkat
- Dargin 2010Dokumen10 halamanDargin 2010Sche Fra MediSiBelum ada peringkat
- Obesity and Bariatric SurgeryDokumen80 halamanObesity and Bariatric SurgerynrkBelum ada peringkat
- Restrictive Lung DisordersDokumen5 halamanRestrictive Lung DisordersSonali RajputBelum ada peringkat
- Absite 2011Dokumen19 halamanAbsite 2011Shawn Robinson0% (1)
- Anaesthesia in Obese PatientsDokumen72 halamanAnaesthesia in Obese PatientsPraveen RamasamyBelum ada peringkat
- Home - Clinical - Management - News - Products - Protocols/Guidelines - Research - Buyer's Guide - Expert Insight - ArchivesDokumen8 halamanHome - Clinical - Management - News - Products - Protocols/Guidelines - Research - Buyer's Guide - Expert Insight - ArchivesDuvvuri SankarBelum ada peringkat
- Acute Respiratory Distress SyndromeDokumen77 halamanAcute Respiratory Distress SyndromeAnnisa Dyah ChairiniBelum ada peringkat
- History of LaparosDokumen27 halamanHistory of LaparosDr. Sanjay KolteBelum ada peringkat
- AtelectasisDokumen28 halamanAtelectasisShikha Acharya100% (1)
- Perioperative Pulmonary Atelectasis - Part II. Clinical Implications Anesthesiology American Society of AnesthesiologistsDokumen78 halamanPerioperative Pulmonary Atelectasis - Part II. Clinical Implications Anesthesiology American Society of Anesthesiologistsrina yulianaBelum ada peringkat
- It 25 - JHP RLDDokumen52 halamanIt 25 - JHP RLDkalajengkingkalakalaBelum ada peringkat
- Acute Respiratory Distress Syndrome, Mechanical Ventilation, and Inhalation Injury in Burn PatientsDokumen13 halamanAcute Respiratory Distress Syndrome, Mechanical Ventilation, and Inhalation Injury in Burn Patientspatriciarreis2991Belum ada peringkat
- Respiratory Disease and AnaesthesiaDokumen8 halamanRespiratory Disease and AnaesthesiaReddyBelum ada peringkat
- Anestesi Laparoskopi Obgyn 123Dokumen27 halamanAnestesi Laparoskopi Obgyn 123Riko RIKBelum ada peringkat
- 1 AppendectomyDokumen16 halaman1 AppendectomyStanford AnesthesiaBelum ada peringkat
- Hypo Ventilation SyndromesDokumen22 halamanHypo Ventilation SyndromesFer45Belum ada peringkat
- Weaning From Mechanical Ventilation: Nizar Eskandar, MD, Michael J. Apostolakos, MDDokumen12 halamanWeaning From Mechanical Ventilation: Nizar Eskandar, MD, Michael J. Apostolakos, MDmartynbbBelum ada peringkat
- Pathophysiology of CopdDokumen62 halamanPathophysiology of CopddrhrshitjainBelum ada peringkat
- Paediatric AnsDokumen142 halamanPaediatric AnsAbdulkadir HasanBelum ada peringkat
- Anesthesia For Laparoscopic SurgeryDokumen38 halamanAnesthesia For Laparoscopic SurgeryMohamed Satti AbdalsadigBelum ada peringkat
- ARDSDokumen55 halamanARDSSandhya HarbolaBelum ada peringkat
- Acute Respiratory Distress SyndromeDokumen43 halamanAcute Respiratory Distress SyndromeAgnes Pritama Fahmi100% (1)
- Obesity and Obstructive Sleep ApnoeaDokumen26 halamanObesity and Obstructive Sleep ApnoeaMagdi PienaarBelum ada peringkat
- PCRJ 201325Dokumen13 halamanPCRJ 201325ashlyn granthamBelum ada peringkat
- Ards 2Dokumen7 halamanArds 2LUCIBELLOT1Belum ada peringkat
- Pulmonary Physical Therapy RevDokumen11 halamanPulmonary Physical Therapy Revpearl042008100% (2)
- Presentation By: DR Prabhakar Moderator: DR DeepakDokumen44 halamanPresentation By: DR Prabhakar Moderator: DR DeepakPrabhakar KumarBelum ada peringkat
- Anesthesia in Laparoscopic Surgery With Intra-Op HypercarbiaDokumen68 halamanAnesthesia in Laparoscopic Surgery With Intra-Op HypercarbiaChalisa アイス 유수Belum ada peringkat
- Mechanical Ventilation in Obese ICU Patients From Intubation To Extubation PDFDokumen8 halamanMechanical Ventilation in Obese ICU Patients From Intubation To Extubation PDFEFE VEBelum ada peringkat
- Robotic ADokumen35 halamanRobotic AMalexandra S CandoBelum ada peringkat
- 318 Surgical Correction of ScoliosisDokumen7 halaman318 Surgical Correction of ScoliosisbangkitayuBelum ada peringkat
- WWW - Cdc.gov/nccdphp/dnpa/obesity/consequences - Htmlpada Tanggal 3 Juni 2014Dokumen4 halamanWWW - Cdc.gov/nccdphp/dnpa/obesity/consequences - Htmlpada Tanggal 3 Juni 2014Dian Istiqamah MardhatillahBelum ada peringkat
- Go To:: Indications For Mechanical VentilationDokumen25 halamanGo To:: Indications For Mechanical VentilationsakuraleeshaoranBelum ada peringkat
- Postoperative Pulmonary ComplicationsDokumen10 halamanPostoperative Pulmonary ComplicationsBadr DihamBelum ada peringkat
- Senior Talk - ARDSDokumen44 halamanSenior Talk - ARDSDrMohammed FouaadBelum ada peringkat
- Acute Respiratory Failure-PRINTDokumen5 halamanAcute Respiratory Failure-PRINTJan SicatBelum ada peringkat
- Anaesthesia For Thoracic Surgery: DR Fazal H KhanDokumen4 halamanAnaesthesia For Thoracic Surgery: DR Fazal H KhanAdeebMutawaBelum ada peringkat
- Article 301574-PrintDokumen17 halamanArticle 301574-PrintRo RyBelum ada peringkat
- Prone in ARDSDokumen27 halamanProne in ARDSEmanuel VidalBelum ada peringkat
- Anglisht 2Dokumen8 halamanAnglisht 2Ejona SuloBelum ada peringkat
- Atelectasis: Go ToDokumen10 halamanAtelectasis: Go Tosuci triana putriBelum ada peringkat
- 09 T016 40473Dokumen15 halaman09 T016 40473Darmawan RizkyBelum ada peringkat
- Rapid Sequence Intubation: BackgroundDokumen8 halamanRapid Sequence Intubation: Backgroundmarsh86Belum ada peringkat
- Cardiovascular & Pulmonary Physiotherapy - WikipediaDokumen13 halamanCardiovascular & Pulmonary Physiotherapy - WikipediaHAMMYER ALROKHAMIBelum ada peringkat
- World's Largest Science, Technology & Medicine Open Access Book PublisherDokumen11 halamanWorld's Largest Science, Technology & Medicine Open Access Book PublisherRabbi'ahBelum ada peringkat
- NeumoperitoneoDokumen42 halamanNeumoperitoneoJohan Vicente MedinaBelum ada peringkat
- Prone Ventilation For Adult Patients With Acute Respiratory Distress Syndrome - UpToDateDokumen19 halamanProne Ventilation For Adult Patients With Acute Respiratory Distress Syndrome - UpToDateHafiz Hari NugrahaBelum ada peringkat
- The Physiologically Difficult Airway: Eview RticleDokumen9 halamanThe Physiologically Difficult Airway: Eview RticleEdson Llerena SalvoBelum ada peringkat
- BPOC TraducereDokumen2 halamanBPOC TraducereMunteanu DragosBelum ada peringkat
- Patophysiology of Lungs ObesityDokumen6 halamanPatophysiology of Lungs ObesityDumitru BiniucBelum ada peringkat
- CDH Modern MXDokumen11 halamanCDH Modern MXphobicmdBelum ada peringkat
- Respiratory EmergenciesDokumen50 halamanRespiratory EmergenciesSandeepa WeerawarnaBelum ada peringkat
- REVIEW Anesthesia For Thoracic Surgery PDFDokumen22 halamanREVIEW Anesthesia For Thoracic Surgery PDFcristinaBelum ada peringkat
- DR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHDokumen47 halamanDR Varsha Atul Shah Senior Consultant Dept of Neonatal and Devt Medicine, SGH Visiting Consultant Dept of Child Devt, KKHJennifer MrjBelum ada peringkat
- Systemic Complications Related To ObesityDokumen2 halamanSystemic Complications Related To ObesityAndres DuranBelum ada peringkat
- Approach To The Patient With Dyspnea - UpToDateDokumen51 halamanApproach To The Patient With Dyspnea - UpToDateWelisson BarbosaBelum ada peringkat
- ARDSDokumen7 halamanARDSSiva SankarBelum ada peringkat
- ANACONDADokumen3 halamanANACONDASiva SankarBelum ada peringkat
- My Garden Class 1Dokumen20 halamanMy Garden Class 1Siva SankarBelum ada peringkat
- Ultrasound Guided Regional Nerve BlocksDokumen32 halamanUltrasound Guided Regional Nerve BlocksSiva SankarBelum ada peringkat
- Sedation and Anesthesia in GI Endoscopy 2008Dokumen12 halamanSedation and Anesthesia in GI Endoscopy 2008Siva SankarBelum ada peringkat
- Perioperative Management of Acquired Hemophilia A: A Case Report and Review of LiteratureDokumen3 halamanPerioperative Management of Acquired Hemophilia A: A Case Report and Review of LiteratureSiva SankarBelum ada peringkat
- H, C Radiolabeled Compounds and Their Applications in Metabolism StudyDokumen5 halamanH, C Radiolabeled Compounds and Their Applications in Metabolism StudySiva SankarBelum ada peringkat
- Statistics - Paediatric SurgeryDokumen9 halamanStatistics - Paediatric SurgerySiva SankarBelum ada peringkat
- SR-JR Leave FormDokumen5 halamanSR-JR Leave FormSiva SankarBelum ada peringkat
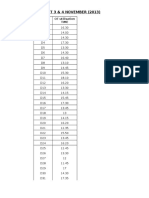
- OT 3 & 4 NOVEMBER (2013) : Date OT Utilisation TimeDokumen4 halamanOT 3 & 4 NOVEMBER (2013) : Date OT Utilisation TimeSiva SankarBelum ada peringkat
- Death SummaryDokumen3 halamanDeath SummarySiva SankarBelum ada peringkat
- Adapted Caprini Score Protocol With Proforma Submitted To JSACDokumen17 halamanAdapted Caprini Score Protocol With Proforma Submitted To JSACSiva SankarBelum ada peringkat
- Glycemic 2010 PDFDokumen9 halamanGlycemic 2010 PDFSiva SankarBelum ada peringkat
- Thromboprophylaxis & RADokumen38 halamanThromboprophylaxis & RASiva SankarBelum ada peringkat
- Systolic Heart FailureDokumen66 halamanSystolic Heart FailureFerinaTarizaIIBelum ada peringkat
- Kerala University of Health Sciences Thrissur: (2010 Scheme)Dokumen1 halamanKerala University of Health Sciences Thrissur: (2010 Scheme)subiBelum ada peringkat
- Vitamin B 12 Fo Late DeficiencyDokumen14 halamanVitamin B 12 Fo Late DeficiencyAnghelo Aldair Velásquez CarrilloBelum ada peringkat
- 5 - O - Shubham BorkarDokumen9 halaman5 - O - Shubham Borkarumapati 1505Belum ada peringkat
- 2-Autoimmune DiseasesDokumen29 halaman2-Autoimmune DiseasessoniaBelum ada peringkat
- ACGME-Accredited Specialties and SubspecialtiesDokumen4 halamanACGME-Accredited Specialties and SubspecialtiesWan Nurul AmieraBelum ada peringkat
- BMI2018Dokumen9 halamanBMI2018jeffordillasBelum ada peringkat
- Drug StudyDokumen3 halamanDrug StudyPauline AñesBelum ada peringkat
- What Is Nutrition?,: Christian NordqvistDokumen2 halamanWhat Is Nutrition?,: Christian NordqvistJunairah Keshia LumabaoBelum ada peringkat
- Biopharmaceutical: What Is A ?Dokumen6 halamanBiopharmaceutical: What Is A ?NarendrakumarBelum ada peringkat
- Pathophysiology - PyelonephritisDokumen2 halamanPathophysiology - PyelonephritisFrancis Kevin Sagudo92% (13)
- PCOL Notes 001 IntroDokumen1 halamanPCOL Notes 001 IntroCansBelum ada peringkat
- Legal Medicine Notes 2020Dokumen8 halamanLegal Medicine Notes 2020Iamharbeyy CastroBelum ada peringkat
- OLHS COVID Phase-IV BackToSchool FlyerDokumen1 halamanOLHS COVID Phase-IV BackToSchool FlyerRachael ThomasBelum ada peringkat
- PMLS ReviewerDokumen6 halamanPMLS ReviewerGBelum ada peringkat
- Overview of Anesthesia - UpToDateDokumen11 halamanOverview of Anesthesia - UpToDateFernandoVianaBelum ada peringkat
- 02 27058Dokumen10 halaman02 27058Gina HyginusBelum ada peringkat
- Rifts - The Complete Skills BookDokumen104 halamanRifts - The Complete Skills BookSgt. Mushroom100% (2)
- Ortopedia Dentofacial Una Vision MultidisciplinariaDokumen1 halamanOrtopedia Dentofacial Una Vision MultidisciplinariaFrancisco Javier GutierrezBelum ada peringkat
- Abdominal TraumaDokumen8 halamanAbdominal Traumahatem alsrour100% (2)
- Cover Letter For MREC ApprovalDokumen2 halamanCover Letter For MREC ApprovalSiti Sakinah Noraladin100% (8)
- Hospital Acquired PneumoniaDokumen48 halamanHospital Acquired PneumoniaKartika RezkyBelum ada peringkat
- Rituximab Tullus Kjeil 2021Dokumen9 halamanRituximab Tullus Kjeil 2021Carmen MunteanBelum ada peringkat
- Acute Glomerulonephritis: Background, Pathophysiology, EtiologyDokumen5 halamanAcute Glomerulonephritis: Background, Pathophysiology, Etiology'Riku' Pratiwie TunaBelum ada peringkat
- Impact of Estrogen Type On Cardiovascular Safety of Combined OralDokumen12 halamanImpact of Estrogen Type On Cardiovascular Safety of Combined OralMary SuescaBelum ada peringkat
- 2 Respiratory TractDokumen39 halaman2 Respiratory TractnanxtoyahBelum ada peringkat
- Assessment of DiaphragmaticDokumen10 halamanAssessment of DiaphragmaticFranco BongiornoBelum ada peringkat
- High Performance Eye Hospital: Shalini Nehra (80) - Sachin Nandanwar (75) - Subhash WagleDokumen45 halamanHigh Performance Eye Hospital: Shalini Nehra (80) - Sachin Nandanwar (75) - Subhash WagleSachin Nandanwar100% (1)
- Health and WellnessDokumen13 halamanHealth and WellnesssumithraBelum ada peringkat
- Reading ListDokumen1 halamanReading ListNosaaliBelum ada peringkat
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomDari EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomPenilaian: 4 dari 5 bintang4/5 (1)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDari EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- Eat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthDari EverandEat Complete: The 21 Nutrients That Fuel Brainpower, Boost Weight Loss, and Transform Your HealthPenilaian: 2 dari 5 bintang2/5 (1)
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainDari EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainPenilaian: 3.5 dari 5 bintang3.5/5 (38)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyDari EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyPenilaian: 4.5 dari 5 bintang4.5/5 (3)
- The Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesDari EverandThe Volumetrics Eating Plan: Techniques and Recipes for Feeling Full on Fewer CaloriesBelum ada peringkat
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonDari EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonPenilaian: 3.5 dari 5 bintang3.5/5 (33)
- The Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoDari EverandThe Stark Naked 21-Day Metabolic Reset: Effortless Weight Loss, Rejuvenating Sleep, Limitless Energy, More MojoBelum ada peringkat
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodDari EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodBelum ada peringkat
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeDari EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeBelum ada peringkat
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarDari EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarPenilaian: 5 dari 5 bintang5/5 (351)
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondDari EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondPenilaian: 4.5 dari 5 bintang4.5/5 (28)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingDari EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingPenilaian: 5 dari 5 bintang5/5 (61)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseDari EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseasePenilaian: 4.5 dari 5 bintang4.5/5 (84)
- Keto Friendly Recipes: Easy Keto For Busy PeopleDari EverandKeto Friendly Recipes: Easy Keto For Busy PeoplePenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossDari EverandThe Complete Beck Diet for Life: The 5-Stage Program for Permanent Weight LossPenilaian: 3.5 dari 5 bintang3.5/5 (6)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodDari EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodPenilaian: 4.5 dari 5 bintang4.5/5 (18)
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossDari EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossPenilaian: 4 dari 5 bintang4/5 (22)
- Smarter Not Harder: The Biohacker's Guide to Getting the Body and Mind You WantDari EverandSmarter Not Harder: The Biohacker's Guide to Getting the Body and Mind You WantPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- Rapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsDari EverandRapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsPenilaian: 5 dari 5 bintang5/5 (7)
- Ultrametabolism: The Simple Plan for Automatic Weight LossDari EverandUltrametabolism: The Simple Plan for Automatic Weight LossPenilaian: 4.5 dari 5 bintang4.5/5 (28)
- Rapid Weight Loss Hypnosis for Women: Self-Hypnosis, Affirmations, and Guided Meditations to Burn Fat, Gastric Band, Eating Habits, Sugar Cravings, Mindfulness, and More.Dari EverandRapid Weight Loss Hypnosis for Women: Self-Hypnosis, Affirmations, and Guided Meditations to Burn Fat, Gastric Band, Eating Habits, Sugar Cravings, Mindfulness, and More.Penilaian: 5 dari 5 bintang5/5 (36)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectDari EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectPenilaian: 3 dari 5 bintang3/5 (5)
- Body Confidence: Venice Nutrition's 3 Step System That Unlocks Your Body's Full PotentialDari EverandBody Confidence: Venice Nutrition's 3 Step System That Unlocks Your Body's Full PotentialPenilaian: 4 dari 5 bintang4/5 (2)
- Good Sugar Bad Sugar: Eat yourself free from sugar and carb addictionDari EverandGood Sugar Bad Sugar: Eat yourself free from sugar and carb addictionPenilaian: 4.5 dari 5 bintang4.5/5 (29)
- Extreme Weight Loss Hypnosis: Self-Hypnosis, Affirmations and Guided Meditations for Burning Fat, Emotional Eating, Food Addiction, Healthy Eating Habits & Mindfulness.Dari EverandExtreme Weight Loss Hypnosis: Self-Hypnosis, Affirmations and Guided Meditations for Burning Fat, Emotional Eating, Food Addiction, Healthy Eating Habits & Mindfulness.Penilaian: 4.5 dari 5 bintang4.5/5 (31)