Anda mungkin juga menyukai
- IHC - InterpretareDokumen185 halamanIHC - InterpretareAnca NeaguBelum ada peringkat
- LNs HNDokumen190 halamanLNs HNNinna Isabel VictorioBelum ada peringkat
- Hodgkins and Non Hodgkins LymphomaDokumen5 halamanHodgkins and Non Hodgkins LymphomakakuBelum ada peringkat
- Molecular - Uniparental Disomy:: NPM1 Frequently Harbors A 4 BP Insertion in LeukemiaDokumen16 halamanMolecular - Uniparental Disomy:: NPM1 Frequently Harbors A 4 BP Insertion in LeukemiaKHBelum ada peringkat
- BoardReviewPart2C MalignantHemePathDokumen184 halamanBoardReviewPart2C MalignantHemePathMaria Cristina Alarcon NietoBelum ada peringkat
- T NK CellDokumen117 halamanT NK CellPpds MtatasuhartaBelum ada peringkat
- Clinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDateDokumen16 halamanClinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDatePablo ZeregaBelum ada peringkat
- Dr. Muhartono, M. Kes, SP - PADokumen108 halamanDr. Muhartono, M. Kes, SP - PAtyahudisaputriBelum ada peringkat
- Pathophysiology NHLDokumen2 halamanPathophysiology NHLPlazer DamasenBelum ada peringkat
- Acute Lymphoblastic Leukemia (ALL)Dokumen14 halamanAcute Lymphoblastic Leukemia (ALL)Med PhuongBelum ada peringkat
- WBC DisordersDokumen114 halamanWBC DisordersNdor BariboloBelum ada peringkat
- Chronic Lymphocytic LeukemiaDokumen54 halamanChronic Lymphocytic LeukemiabassamhematolBelum ada peringkat
- Acute and Chronic LeukemiasDokumen3 halamanAcute and Chronic Leukemiaskaku100% (2)
- Answers - Haematological Malignancies Digital Images QuizDokumen4 halamanAnswers - Haematological Malignancies Digital Images Quizcande casanasBelum ada peringkat
- Leukemias and Lymphomas Flow Chart ModifiedDokumen5 halamanLeukemias and Lymphomas Flow Chart Modifiedlovelyc95Belum ada peringkat
- MK Hematology-LeukemiasDokumen35 halamanMK Hematology-LeukemiasMoses Jr KazevuBelum ada peringkat
- Acut e Lymphoblastic Leukemia: Mihaela OnciuDokumen20 halamanAcut e Lymphoblastic Leukemia: Mihaela OnciuSyamsu Akbar KhairillahBelum ada peringkat
- Chronic Lymphocytic CLLDokumen14 halamanChronic Lymphocytic CLLPamy AbellaBelum ada peringkat
- Leucemia Limfatica CronicaDokumen18 halamanLeucemia Limfatica CronicaUngureanu Andrei100% (1)
- Sam CD Rom - ImmunologyDokumen111 halamanSam CD Rom - ImmunologyDr. Muha. Hasan Mahbub-Ur-RahmanBelum ada peringkat
- CDDokumen32 halamanCDHorga LucianBelum ada peringkat
- Origin of Lymphoid Neoplasms: CLP: BLB: NBC: MC: GC: MZDokumen26 halamanOrigin of Lymphoid Neoplasms: CLP: BLB: NBC: MC: GC: MZSri Naharindah NingBelum ada peringkat
- Hematopatologie 2016Dokumen45 halamanHematopatologie 2016CristiBelum ada peringkat
- BoardReviewPart2B MalignantHemePathDokumen207 halamanBoardReviewPart2B MalignantHemePathMaria Cristina Alarcon NietoBelum ada peringkat
- PUB221 FlowCytom SampleDokumen12 halamanPUB221 FlowCytom SampleDaryl FootBelum ada peringkat
- Hodgkin'S Disease AND Non-Hodgkin'S LymphomaDokumen42 halamanHodgkin'S Disease AND Non-Hodgkin'S LymphomaRayya TriandaBelum ada peringkat
- 20 Lymphomas and LeukemiastextsDokumen40 halaman20 Lymphomas and LeukemiastextsArief SeptianurBelum ada peringkat
- Chapter 13 Neoplastic Proliferations of White CellsDokumen16 halamanChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- Hemat 3 Notes 4the Chronic Lymphocytic Leukemias and LymphomaDokumen11 halamanHemat 3 Notes 4the Chronic Lymphocytic Leukemias and LymphomaAadya RoshanBelum ada peringkat
- Acute Leukaemia-Update: DR Niranjan N. RathodDokumen89 halamanAcute Leukaemia-Update: DR Niranjan N. RathodratanBelum ada peringkat
- List of Human Clusters of DifferentiationDokumen22 halamanList of Human Clusters of DifferentiationMaryam ShahrasbiBelum ada peringkat
- ALL - Curs (Engl)Dokumen10 halamanALL - Curs (Engl)Andreea TudurachiBelum ada peringkat
- ადამიანის CD ანტიგენებიDokumen1 halamanადამიანის CD ანტიგენებიEMD GROUP100% (1)
- AML, CML, ALL, CLL, HemophiliaDokumen7 halamanAML, CML, ALL, CLL, HemophiliaJamara Kyla Dela CruzBelum ada peringkat
- Acute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMDokumen52 halamanAcute Leukemia: DR Rosline Hassan Hematology Department School of Medical Sciences USMJamilBelum ada peringkat
- Clasificacion de Linfomas BDokumen25 halamanClasificacion de Linfomas BFiorella SalvatBelum ada peringkat
- The WHO-EORTC ClassificationDokumen17 halamanThe WHO-EORTC ClassificationLagavulin2Belum ada peringkat
- Leukemias & Lymphomas - HY USMLEDokumen87 halamanLeukemias & Lymphomas - HY USMLEMatt McGlothlinBelum ada peringkat
- CD MneumonicDokumen9 halamanCD Mneumonicgaa5Belum ada peringkat
- AML WHO IncludedDokumen79 halamanAML WHO IncludedErika Nicole DoradoBelum ada peringkat
- Ahmad Sh. Silmi MSC Haematology, FIBMSDokumen63 halamanAhmad Sh. Silmi MSC Haematology, FIBMSHadi AdamBelum ada peringkat
- HaematologyDokumen25 halamanHaematologyMenziPhiwokuhleSukatiBelum ada peringkat
- All Aml NCCN 2023 HamidahDokumen45 halamanAll Aml NCCN 2023 HamidahPPDS IPD ULMBelum ada peringkat
- LLC 2006Dokumen11 halamanLLC 2006claudia8a_ulamedBelum ada peringkat
- Limfoproliferari Cronice MaligneDokumen18 halamanLimfoproliferari Cronice MaligneAlice MuscaBelum ada peringkat
- GRANULOPOIESIS (Autosaved) .PPTX OKLADokumen93 halamanGRANULOPOIESIS (Autosaved) .PPTX OKLAPrincewill SeiyefaBelum ada peringkat
- Pa Tho Physiology of LymphomasDokumen17 halamanPa Tho Physiology of LymphomasKent MasadoBelum ada peringkat
- 2.cells of Immune System Notes PowerpointDokumen34 halaman2.cells of Immune System Notes Powerpointt4ths999Belum ada peringkat
- Cluster of Differentiation Antigen PosterDokumen1 halamanCluster of Differentiation Antigen PosterReeti R. Bhat100% (1)
- Hodgkin's DiseaseDokumen58 halamanHodgkin's Diseasealibayaty1Belum ada peringkat
- Lymph Node CytologyDokumen39 halamanLymph Node Cytologykamranghani641Belum ada peringkat
- 25 Yo Male With Fever of 1month Duration HB 5.0gm/dl TLC: 70,000 Cells/cumm Platelets: 40,000/cummDokumen47 halaman25 Yo Male With Fever of 1month Duration HB 5.0gm/dl TLC: 70,000 Cells/cumm Platelets: 40,000/cummMahalakshmi PalanisamiBelum ada peringkat
- Matute SDokumen5 halamanMatute SLUCASBelum ada peringkat
- Acute Lymphoblastic LeukemiaDokumen5 halamanAcute Lymphoblastic LeukemiavnykumalasariBelum ada peringkat
- Hematology DiseasesDokumen4 halamanHematology DiseasesLeonida DalugdogBelum ada peringkat
- Advances in Management of NHLDokumen34 halamanAdvances in Management of NHLMohammed Abd ElfattahBelum ada peringkat
- Aggressive T - Cell Lymphomas 2021 UpdatesDokumen41 halamanAggressive T - Cell Lymphomas 2021 UpdatesAnnaBelum ada peringkat
- Pathology SWTDokumen4 halamanPathology SWTkishorechandraBelum ada peringkat
- I'm So Stressed InfographicDokumen1 halamanI'm So Stressed InfographicBrett FieldsBelum ada peringkat
- Things You Should Know About StressDokumen2 halamanThings You Should Know About StressBrett FieldsBelum ada peringkat
- Brainactivitybook PDFDokumen17 halamanBrainactivitybook PDFBrett FieldsBelum ada peringkat
- Im So Stressed OutDokumen2 halamanIm So Stressed OutBrett FieldsBelum ada peringkat
- Scene 5 - 2nd RevisionDokumen3 halamanScene 5 - 2nd RevisionBrett FieldsBelum ada peringkat
- Slow Jam Hold On Riff Procrastiplayers Wednesday Night Jam Amazon G Jam I Wanna I Ain't Got It Grooveman Nothing But The Funk I Wanna Get in ItDokumen1 halamanSlow Jam Hold On Riff Procrastiplayers Wednesday Night Jam Amazon G Jam I Wanna I Ain't Got It Grooveman Nothing But The Funk I Wanna Get in ItBrett FieldsBelum ada peringkat
- Nephrin (Protein in Slit Diaphragm of Podocytes) Plays An Essential Role in TheDokumen3 halamanNephrin (Protein in Slit Diaphragm of Podocytes) Plays An Essential Role in TheBrett FieldsBelum ada peringkat
- HormonesDokumen48 halamanHormonesBrett FieldsBelum ada peringkat
- Common Drugs ListDokumen3 halamanCommon Drugs ListBrett FieldsBelum ada peringkat
- Nephrin (Protein in Slit Diaphragm of Podocytes) Plays An Essential Role in TheDokumen3 halamanNephrin (Protein in Slit Diaphragm of Podocytes) Plays An Essential Role in TheBrett FieldsBelum ada peringkat
- Behaviors (Evidenced by The Analysis Results Below)Dokumen2 halamanBehaviors (Evidenced by The Analysis Results Below)Brett FieldsBelum ada peringkat
- Notification of Housing AllowanceDokumen1 halamanNotification of Housing AllowanceBrett FieldsBelum ada peringkat
- Boardcommittee Meeting AgendaDokumen1 halamanBoardcommittee Meeting AgendaBrett FieldsBelum ada peringkat
- Urology Smart PhrasesDokumen1 halamanUrology Smart PhrasesBrett FieldsBelum ada peringkat
- Gene Therapy Challenges and SuccessDokumen5 halamanGene Therapy Challenges and SuccessEditor IJTSRDBelum ada peringkat
- Cardiovascular Pharmacotherapeutics PDFDokumen798 halamanCardiovascular Pharmacotherapeutics PDFMaria del Pilar Devis MoralesBelum ada peringkat
- Collagen: RD RDDokumen12 halamanCollagen: RD RDrupali100% (1)
- Computational Methods For GPCR Drug Discovery PDFDokumen437 halamanComputational Methods For GPCR Drug Discovery PDFShin KaojuBelum ada peringkat
- XI Botany ChapterWise Prvs Questions HssliveDokumen25 halamanXI Botany ChapterWise Prvs Questions Hsslivejithu63% (8)
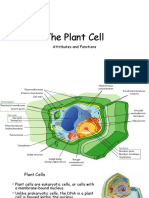
- The Plant CellDokumen30 halamanThe Plant CellMichael GentilesBelum ada peringkat
- IAL Edexcel Biology Unit 2 RevisionDokumen11 halamanIAL Edexcel Biology Unit 2 RevisionWillie WongBelum ada peringkat
- Meiosis and Sexual ReproductionDokumen48 halamanMeiosis and Sexual Reproductionerdayu86100% (1)
- Enzymes Proteins ESqDokumen26 halamanEnzymes Proteins ESqBihandu PigeraBelum ada peringkat
- A&p - All Files in One PDFDokumen52 halamanA&p - All Files in One PDFSreejith Jagal KishoreBelum ada peringkat
- Ana Physio 1prelims 2021-22 1stsem 1B - ExamDokumen5 halamanAna Physio 1prelims 2021-22 1stsem 1B - ExamKwenzie FortalezaBelum ada peringkat
- PF General TalkDokumen61 halamanPF General TalkindrahermawanBelum ada peringkat
- Molecular Cell Biology Lodish 6th Edition Test BankDokumen36 halamanMolecular Cell Biology Lodish 6th Edition Test Bankproachbechancerfhu100% (31)
- Dna Replication and Protein Synthesis Lesson PlanDokumen10 halamanDna Replication and Protein Synthesis Lesson Planapi-356227663100% (2)
- Pharmacology of Renin-Angiotensin-System Blockers and COVID-19: Confusion Around ACE2Dokumen3 halamanPharmacology of Renin-Angiotensin-System Blockers and COVID-19: Confusion Around ACE2Sharan SahotaBelum ada peringkat
- Melaka BoosterDokumen12 halamanMelaka BoosterHaifa amirahBelum ada peringkat
- Daily Lesson Plan-Biology Grade 8Dokumen9 halamanDaily Lesson Plan-Biology Grade 8Zhaine MendozaBelum ada peringkat
- Principles of Animal DevelopmentDokumen42 halamanPrinciples of Animal Developmentrifan elyBelum ada peringkat
- Artepillin C As An Outstanding Phenolic Compound of Brazilian Green Propolis For Disease Treatment: A Review On Pharmacological AspectsDokumen13 halamanArtepillin C As An Outstanding Phenolic Compound of Brazilian Green Propolis For Disease Treatment: A Review On Pharmacological AspectslyviaBelum ada peringkat
- Cell Cycle and Cell DivisionDokumen8 halamanCell Cycle and Cell Divisionbhupeshgalani100% (2)
- Benzopyrene Exposure Disrupts DNA Methylation and Growth DynamicsDokumen11 halamanBenzopyrene Exposure Disrupts DNA Methylation and Growth DynamicsLorena IntriagoBelum ada peringkat
- Biology Esei STPM 2017@ 2018Dokumen43 halamanBiology Esei STPM 2017@ 2018Wei Yuen100% (1)
- 5.2 AssignmentDokumen2 halaman5.2 Assignmentannie bungisngisBelum ada peringkat
- Osmosis in Potato StripsDokumen2 halamanOsmosis in Potato StripsBritneyBelum ada peringkat
- Glycolysis Ch.14Dokumen51 halamanGlycolysis Ch.14Yousef KhallafBelum ada peringkat
- Alveolar Soft Part SarcomaDokumen4 halamanAlveolar Soft Part Sarcomanohemi9Belum ada peringkat
- WJEC Markscheme Gce Ms Biology Jun09legacy eDokumen34 halamanWJEC Markscheme Gce Ms Biology Jun09legacy eEmi JiHyeon KimBelum ada peringkat
- IMMUNITYDokumen58 halamanIMMUNITYkamala 123Belum ada peringkat
- EPITHELIUMDokumen38 halamanEPITHELIUMAstridBelum ada peringkat
- M - 114 Second Messenger in The Hormone ActionDokumen3 halamanM - 114 Second Messenger in The Hormone ActionDr. Tapan Kr. DuttaBelum ada peringkat