Anda mungkin juga menyukai
- 234 585 1 PBDokumen7 halaman234 585 1 PBlisa chanBelum ada peringkat
- Hachiko StuteDokumen6 halamanHachiko Stutelisa chanBelum ada peringkat
- Analysis of General and Oral Quality of Life and Satisfaction With Treatment Among Anticoagulated PatientsDokumen4 halamanAnalysis of General and Oral Quality of Life and Satisfaction With Treatment Among Anticoagulated Patientslisa chanBelum ada peringkat
- Rashid IchsanDokumen4 halamanRashid Ichsanlisa chanBelum ada peringkat
- Hachiko StuteDokumen6 halamanHachiko Stutelisa chanBelum ada peringkat
- Bleaching ReviewDokumen14 halamanBleaching ReviewAbhisek DasBelum ada peringkat
- Chapter 11 The Dental Surveyor and Its UsesDokumen4 halamanChapter 11 The Dental Surveyor and Its UsesSantosh AgarwalBelum ada peringkat
- 2 4 15-20Dokumen6 halaman2 4 15-20lisa chanBelum ada peringkat
- Reling Rebasing 1Dokumen45 halamanReling Rebasing 1lisa chanBelum ada peringkat
- Hachiko StuteDokumen6 halamanHachiko Stutelisa chanBelum ada peringkat
- Prosthodontic DiagnosisDokumen15 halamanProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
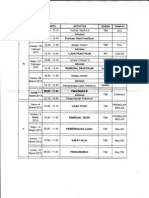
- Ikgd Blokv: Jadwal Perkuliahan TutorialDokumen1 halamanIkgd Blokv: Jadwal Perkuliahan Tutoriallisa chanBelum ada peringkat
- Hachiko StuteDokumen6 halamanHachiko Stutelisa chanBelum ada peringkat
- Hachiko StuteDokumen6 halamanHachiko Stutelisa chanBelum ada peringkat
- Jurnal PH PDFDokumen15 halamanJurnal PH PDFason10Belum ada peringkat
- Jadwal Kuliah-Lembar 3Dokumen1 halamanJadwal Kuliah-Lembar 3lisa chanBelum ada peringkat
- Hachiko StuteDokumen5 halamanHachiko Stutelisa chanBelum ada peringkat
- Tugas Bahasa Inggris Nama: Lidya Kelas: XDDokumen6 halamanTugas Bahasa Inggris Nama: Lidya Kelas: XDlisa chanBelum ada peringkat
- Dentinogenesis: Dr. Asmat Jameel Assistant Professor B.D.S, F.C.P.S Head Department of Oral BiologyDokumen17 halamanDentinogenesis: Dr. Asmat Jameel Assistant Professor B.D.S, F.C.P.S Head Department of Oral Biologylisa chanBelum ada peringkat
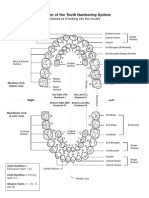
- Diagram of The Tooth Numbering SystemDokumen1 halamanDiagram of The Tooth Numbering Systemsaleh900Belum ada peringkat
- Hachiko StuteDokumen6 halamanHachiko Stutelisa chanBelum ada peringkat
- Excel (Laporan Praktikum 4)Dokumen16 halamanExcel (Laporan Praktikum 4)lisa chanBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Eb4069135 F enDokumen13 halamanEb4069135 F enkalvino314Belum ada peringkat
- Chefs at HomeDokumen4 halamanChefs at Homezbdv2kyzv7Belum ada peringkat
- Ben Wilkins PRISON MADNESS and LOVE LETTERS: THE LOST ARTDokumen5 halamanBen Wilkins PRISON MADNESS and LOVE LETTERS: THE LOST ARTBarbara BergmannBelum ada peringkat
- SPECIFIC GRAVITY - DENSITY OF HYDRAULIC CEMENT (IS - 4031-Part 11-1988)Dokumen6 halamanSPECIFIC GRAVITY - DENSITY OF HYDRAULIC CEMENT (IS - 4031-Part 11-1988)Pritha DasBelum ada peringkat
- AWWA M28 Rehabilitation of Water Mains 3rd Ed 2014Dokumen133 halamanAWWA M28 Rehabilitation of Water Mains 3rd Ed 2014millini67% (3)
- Etabloc Technical DataDokumen108 halamanEtabloc Technical Dataedward ksbBelum ada peringkat
- Anhydrous Ammonia Unloading Station & Storage/Vaporizer SystemDokumen2 halamanAnhydrous Ammonia Unloading Station & Storage/Vaporizer SystemWalter Rigamonti100% (1)
- Evolis User ManualDokumen28 halamanEvolis User ManualIonmadalin1000Belum ada peringkat
- Fossil Fuel and The Environment PPT Project FinalDokumen14 halamanFossil Fuel and The Environment PPT Project Finalapi-298052133Belum ada peringkat
- Sharp LC 50le440u ProspectoDokumen2 halamanSharp LC 50le440u ProspectovwcxlBelum ada peringkat
- 2021 Vallourec Universal Registration DocumentDokumen368 halaman2021 Vallourec Universal Registration DocumentRolando Jara YoungBelum ada peringkat
- Verbal ReasoningDokumen8 halamanVerbal ReasoningyasirBelum ada peringkat
- BR A Consumables Catalog ElecDokumen31 halamanBR A Consumables Catalog Elecdweil1552Belum ada peringkat
- Final Project Proposal Digital Stopwatch-1Dokumen6 halamanFinal Project Proposal Digital Stopwatch-1Shahid AbbasBelum ada peringkat
- LP Pressure TestingDokumen34 halamanLP Pressure TestinglisaBelum ada peringkat
- 2206 - Stamina Monograph - 0 PDFDokumen3 halaman2206 - Stamina Monograph - 0 PDFMhuez Iz Brave'sBelum ada peringkat
- Caterpillar 360 KWDokumen6 halamanCaterpillar 360 KWAde WawanBelum ada peringkat
- Development of The FaceDokumen76 halamanDevelopment of The Facedr parveen bathla100% (1)
- Moisture ManagementDokumen5 halamanMoisture ManagementSombis2011Belum ada peringkat
- Traxonecue Catalogue 2011 Revise 2 Low Res Eng (4!5!2011)Dokumen62 halamanTraxonecue Catalogue 2011 Revise 2 Low Res Eng (4!5!2011)Wilson ChimBelum ada peringkat
- Unit-2 Final KshitijDokumen108 halamanUnit-2 Final KshitijShubham JainBelum ada peringkat
- Railway Electrification Projects Budget 2019-20Dokumen9 halamanRailway Electrification Projects Budget 2019-20Muhammad Meraj AlamBelum ada peringkat
- October 14, 2011 Strathmore TimesDokumen28 halamanOctober 14, 2011 Strathmore TimesStrathmore TimesBelum ada peringkat
- WPS Ernicu 7 R1 3 6 PDFDokumen4 halamanWPS Ernicu 7 R1 3 6 PDFandresBelum ada peringkat
- Hypnotherapy GuideDokumen48 halamanHypnotherapy Guides_e_bell100% (2)
- RESISTANCEDokumen9 halamanRESISTANCERohit SahuBelum ada peringkat
- Vedic Astrology OverviewDokumen1 halamanVedic Astrology Overviewhuman999100% (8)
- Management of Septic Shock in An Intermediate Care UnitDokumen20 halamanManagement of Septic Shock in An Intermediate Care UnitJHBelum ada peringkat
- Radiesse Pálpebras Gox-8-E2633Dokumen7 halamanRadiesse Pálpebras Gox-8-E2633Camila CrosaraBelum ada peringkat
- 43-101 Technical Report Quimsacocha, February 2009Dokumen187 halaman43-101 Technical Report Quimsacocha, February 2009Marco Vinicio SotoBelum ada peringkat