Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
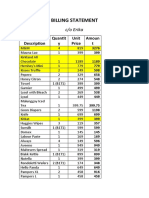
- S&R - Billing StatementDokumen4 halamanS&R - Billing StatementCzara DyBelum ada peringkat
- Scra 2014Dokumen3 halamanScra 2014Czara DyBelum ada peringkat
- Barcelote Vs - RepublicDokumen2 halamanBarcelote Vs - RepublicCzara DyBelum ada peringkat
- CORPPPPPPPOOOOOOOOODokumen2 halamanCORPPPPPPPOOOOOOOOOCzara DyBelum ada peringkat
- Marie Ivonne F. Reyes: Pasig Catholic SchoolDokumen1 halamanMarie Ivonne F. Reyes: Pasig Catholic SchoolCzara DyBelum ada peringkat
- Castillo vs. RepublicDokumen2 halamanCastillo vs. RepublicCzara DyBelum ada peringkat
- BlaaaaaaaahDokumen1 halamanBlaaaaaaaahCzara DyBelum ada peringkat
- Republic Vs de GraciaDokumen5 halamanRepublic Vs de GraciaRuiz Arenas AgacitaBelum ada peringkat
- Republic Vs de GraciaDokumen5 halamanRepublic Vs de GraciaRuiz Arenas AgacitaBelum ada peringkat
- Barcelote Vs - RepublicDokumen2 halamanBarcelote Vs - RepublicCzara DyBelum ada peringkat
- Corpo Notes 2018 PrelimsDokumen14 halamanCorpo Notes 2018 PrelimsCzara DyBelum ada peringkat
- Lacerna Vs CorcinoDokumen2 halamanLacerna Vs CorcinobenBelum ada peringkat
- Garcia vs. RecioDokumen2 halamanGarcia vs. RecioCzara DyBelum ada peringkat
- Corpo PrelimsDokumen67 halamanCorpo PrelimsCzara DyBelum ada peringkat
- G.R. No. L-48955, June 30, 1987)Dokumen8 halamanG.R. No. L-48955, June 30, 1987)Czara DyBelum ada peringkat
- Bank Wins Property CaseDokumen2 halamanBank Wins Property CaseCzara DyBelum ada peringkat
- Banking Mon 7718Dokumen2 halamanBanking Mon 7718Czara DyBelum ada peringkat
- Fujiki vs. MarinayDokumen2 halamanFujiki vs. MarinayCzara DyBelum ada peringkat
- G.R. No. L-48955, June 30, 1987)Dokumen8 halamanG.R. No. L-48955, June 30, 1987)Czara DyBelum ada peringkat
- Sunio v. NLRC: Corporation's Separate Juridical PersonalityDokumen3 halamanSunio v. NLRC: Corporation's Separate Juridical PersonalityCzara DyBelum ada peringkat
- Page 7 - 8 Proximate or Legal Cause To Legal InjuryDokumen12 halamanPage 7 - 8 Proximate or Legal Cause To Legal InjuryCzara DyBelum ada peringkat
- Bank Wins Property CaseDokumen2 halamanBank Wins Property CaseCzara DyBelum ada peringkat
- Jimenez vs. FranciscoDokumen1 halamanJimenez vs. FranciscoCzara DyBelum ada peringkat
- Torts Finals Pages 15-19Dokumen3 halamanTorts Finals Pages 15-19Czara DyBelum ada peringkat
- Nil Cases FinalsDokumen37 halamanNil Cases FinalsCzara DyBelum ada peringkat
- PNB Vs CA DigestDokumen3 halamanPNB Vs CA DigestCzara DyBelum ada peringkat
- Institution of Heirs. It Will Not Result To IntestacyDokumen9 halamanInstitution of Heirs. It Will Not Result To IntestacyCzara DyBelum ada peringkat
- Evidence PPT 2018 - Dy NotesDokumen14 halamanEvidence PPT 2018 - Dy NotesCzara DyBelum ada peringkat
- Proximate or Legal Cause To Legal InjuryDokumen12 halamanProximate or Legal Cause To Legal InjuryCzara DyBelum ada peringkat
- Q&A Wills Dean AligadaDokumen5 halamanQ&A Wills Dean AligadaCzara DyBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Infant Sleep and Its Relation With CognitionDokumen15 halamanInfant Sleep and Its Relation With CognitionLara GintingBelum ada peringkat
- Presentation by Prof Katya Rubia - The Change Within: Sustainable Effects Ofsustainable Effects of Meditation On Healthmeditation On HealthDokumen24 halamanPresentation by Prof Katya Rubia - The Change Within: Sustainable Effects Ofsustainable Effects of Meditation On Healthmeditation On Healthtanaha100% (3)
- SeeingStars Lesson PlanDokumen11 halamanSeeingStars Lesson PlanMaria Maqsoudi-KarimiBelum ada peringkat
- Psychological Processes in Language Learning and Teaching: Methods and Approaches of PsycholinguisticsDokumen7 halamanPsychological Processes in Language Learning and Teaching: Methods and Approaches of PsycholinguisticsMohamed IZZ El-DeenBelum ada peringkat
- Psychoeducational Assessment Page ContentDokumen2 halamanPsychoeducational Assessment Page Contentapi-691702370Belum ada peringkat
- Dissolution Language LossDokumen3 halamanDissolution Language LossyulianaBelum ada peringkat
- A Materialist Theory of The Mind by D. M. ArmstrongDokumen8 halamanA Materialist Theory of The Mind by D. M. ArmstrongDon ArthurBelum ada peringkat
- Unit 9b Listening p143 Audio ScriptDokumen1 halamanUnit 9b Listening p143 Audio ScriptふんBelum ada peringkat
- Brain Structure and FunctionDokumen4 halamanBrain Structure and FunctionTenri FaniBelum ada peringkat
- Learning Neural Activations: Fayyaz Ul Amir Afsar Minhas and Amina AsifDokumen10 halamanLearning Neural Activations: Fayyaz Ul Amir Afsar Minhas and Amina AsifssrefrBelum ada peringkat
- Conceptual FrameworkDokumen10 halamanConceptual FrameworkMeynard AndresBelum ada peringkat
- Gustatory SystemDokumen32 halamanGustatory SystemGalih Wahyu SaputraBelum ada peringkat
- Psychological Assessment Fifth EditionDokumen15 halamanPsychological Assessment Fifth EditionDiky Derriansyah20% (5)
- What Is The Difference Between Second Language and Foreign Language LearningDokumen4 halamanWhat Is The Difference Between Second Language and Foreign Language Learningjhasmin rose avellanaBelum ada peringkat
- Verbal Creativity ReportDokumen4 halamanVerbal Creativity Reportjesellebalines3Belum ada peringkat
- Theory of Personality Chapter-1Dokumen13 halamanTheory of Personality Chapter-1chat gaza0% (1)
- Individual Behaviour in ObDokumen163 halamanIndividual Behaviour in ObIgdtuw100% (1)
- Relationship between personality traits and logical intelligenceDokumen7 halamanRelationship between personality traits and logical intelligenceMae VerniceBelum ada peringkat
- GROUP 3'S IQ AND INTELLIGENCEDokumen17 halamanGROUP 3'S IQ AND INTELLIGENCEAngel ClerigoBelum ada peringkat
- Artificial Intelligence ExplainedDokumen17 halamanArtificial Intelligence ExplainedRohit RawatBelum ada peringkat
- Personal DevelopmewntDokumen14 halamanPersonal DevelopmewntKeneth Rose FagtananBelum ada peringkat
- ModuleDokumen8 halamanModuleMerry Joy Tauro Libo-onBelum ada peringkat
- Nature Vs NurtureDokumen7 halamanNature Vs NurtureDeepaPandeyBelum ada peringkat
- Adults Tool KitDokumen30 halamanAdults Tool KitCamila Constanza Soto EspinozaBelum ada peringkat
- (NLP For Education) Richard Bandler - Kate Benson - Teaching Excellence - The Definitive Guide To NLP For Teaching and Learning-New Thinking Publications (2018) PDFDokumen433 halaman(NLP For Education) Richard Bandler - Kate Benson - Teaching Excellence - The Definitive Guide To NLP For Teaching and Learning-New Thinking Publications (2018) PDFmuveszszi100% (20)
- Facilitating Learner - Centered TeachingDokumen21 halamanFacilitating Learner - Centered TeachingRicamae BalmesBelum ada peringkat
- Orr Transferencecountertransference 1954 PDFDokumen51 halamanOrr Transferencecountertransference 1954 PDFLuiz Fernando Fontes-TeixeiraBelum ada peringkat
- Holistic Nursing Care ModelDokumen14 halamanHolistic Nursing Care ModelmujionoBelum ada peringkat
- Clinical Psychology Notes No. 1Dokumen2 halamanClinical Psychology Notes No. 1Jerine Bonus ApostolBelum ada peringkat
- The Intelligence Trap - David RobsonDokumen312 halamanThe Intelligence Trap - David RobsonmichealangeloBelum ada peringkat