Anda mungkin juga menyukai
- Q1. (A) The Diagram Shows A Microphone Being Used To Detect The Output From ADokumen10 halamanQ1. (A) The Diagram Shows A Microphone Being Used To Detect The Output From ASivmi MalishaBelum ada peringkat
- Outlook 2Dokumen188 halamanOutlook 2Mafer Garces NeuhausBelum ada peringkat
- Goals in LifeDokumen4 halamanGoals in LifeNessa Layos MorilloBelum ada peringkat
- Bacterial Genome Assembly IlluminaDokumen49 halamanBacterial Genome Assembly IlluminadksaBelum ada peringkat
- Management of Preterm LaborDokumen2 halamanManagement of Preterm LaborpolygoneBelum ada peringkat
- Itc LimitedDokumen64 halamanItc Limitedjulee G0% (1)
- Quality of Life of Elderly With Chronic Liver DiseasesDokumen7 halamanQuality of Life of Elderly With Chronic Liver DiseasesIOSRjournalBelum ada peringkat
- Compartment SyndromeDokumen14 halamanCompartment SyndromedokteraanBelum ada peringkat
- Expo Cervantes 2Dokumen31 halamanExpo Cervantes 2Alfredo Nano VieyraBelum ada peringkat
- Abdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduDokumen4 halamanAbdominal Tuberculosis in Nepal Medical College Teaching Hospital, KathmanduSavitri Maharani BudimanBelum ada peringkat
- Preventive Medicine: Contents Lists Available atDokumen5 halamanPreventive Medicine: Contents Lists Available atYenza FaheraBelum ada peringkat
- Acute Cholecystitis: From ER To Surgery: Riginal RticleDokumen5 halamanAcute Cholecystitis: From ER To Surgery: Riginal RticleKrystel Joy AuroBelum ada peringkat
- Relationship Between Body Mass Index and Length of Hospital Stay For Gallbladder DiseaseDokumen6 halamanRelationship Between Body Mass Index and Length of Hospital Stay For Gallbladder DiseaseAmitesh AnandBelum ada peringkat
- 1749-7922-6-37 - SalinDokumen5 halaman1749-7922-6-37 - SalinAnonymous InJS6aYZBelum ada peringkat
- Cholelithiasis: Causative Factors, Clinical Manifestations and ManagementDokumen6 halamanCholelithiasis: Causative Factors, Clinical Manifestations and ManagementmusdalifahBelum ada peringkat
- Etiology, Treatment Outcome and Prognostic Factors Among Patients With Secondary Peritonitis at Bugando Medical Centre, Mwanza, TanzaniaDokumen13 halamanEtiology, Treatment Outcome and Prognostic Factors Among Patients With Secondary Peritonitis at Bugando Medical Centre, Mwanza, Tanzaniayossy aciBelum ada peringkat
- 4 Murali Et AlDokumen4 halaman4 Murali Et AleditorijmrhsBelum ada peringkat
- Mortality in Typhoid Intestinal Perforation-A Declining TrendDokumen3 halamanMortality in Typhoid Intestinal Perforation-A Declining Trendaura009Belum ada peringkat
- Choledochal CystDokumen5 halamanCholedochal CystZulia Ahmad BurhaniBelum ada peringkat
- Alcohol Consumption and Risk of Colon Cancer: Evidence From The National Health and Nutrition Examination Survey I Epidemiologic Follow-Up StudyDokumen10 halamanAlcohol Consumption and Risk of Colon Cancer: Evidence From The National Health and Nutrition Examination Survey I Epidemiologic Follow-Up StudyIra FerawatiBelum ada peringkat
- Hum. Reprod.-2013-Romosan-1569-79Dokumen11 halamanHum. Reprod.-2013-Romosan-1569-79Ahmad Arbi AninditoBelum ada peringkat
- Sumar Lucrari MarisiensisDokumen103 halamanSumar Lucrari MarisiensisHumaMihaiBelum ada peringkat
- Inflammatory Potential of Diet and Risk of Colorectal Cancer A Casecontrol Study From ItalyDokumen7 halamanInflammatory Potential of Diet and Risk of Colorectal Cancer A Casecontrol Study From ItalyHenrique VidalBelum ada peringkat
- Intestinal Tuberculosis: A Diagnostic Challenge: © 2017 John Wiley & Sons LTDDokumen6 halamanIntestinal Tuberculosis: A Diagnostic Challenge: © 2017 John Wiley & Sons LTDLily SmithBelum ada peringkat
- Clinical Outcome in Children With Chronic Recurrent Multifocal OsteomyelitisDokumen4 halamanClinical Outcome in Children With Chronic Recurrent Multifocal OsteomyelitisJiwo SaciladhBelum ada peringkat
- Cancer - 2010 - Italiano - Trends in Survival For Patients With Metastatic Soft Tissue SarcomaDokumen6 halamanCancer - 2010 - Italiano - Trends in Survival For Patients With Metastatic Soft Tissue SarcomaAna LimeiraBelum ada peringkat
- Colorectal Carcinoma: A Six Years Experience at A Tertiary Care Hospital of SindhDokumen3 halamanColorectal Carcinoma: A Six Years Experience at A Tertiary Care Hospital of SindhShahimulk KhattakBelum ada peringkat
- Colovesical FistulaDokumen6 halamanColovesical FistulaJdloyerBelum ada peringkat
- ArticuloDokumen9 halamanArticuloElyzabeth BonnesBelum ada peringkat
- A Clinical Study On Extrapulmonary TuberculosiDokumen10 halamanA Clinical Study On Extrapulmonary TuberculosinayemamasruraBelum ada peringkat
- Development of Type I Gastric Carcinoid in Patients With Chronic Atrophic GastritisDokumen9 halamanDevelopment of Type I Gastric Carcinoid in Patients With Chronic Atrophic GastritisAbristaSeptikasariBelum ada peringkat
- Healthmed 15 1 Damir SecicDokumen6 halamanHealthmed 15 1 Damir SecicEdoHBelum ada peringkat
- The New England Journal of MedicineDokumen12 halamanThe New England Journal of MedicineElyzabeth BonnesBelum ada peringkat
- Disparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsDokumen5 halamanDisparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsKristelle HernandezBelum ada peringkat
- Annsurg00166 0011Dokumen8 halamanAnnsurg00166 0011Muhammad FadillahBelum ada peringkat
- Paper05 Jan-Jun2007Dokumen6 halamanPaper05 Jan-Jun2007cystanarisaBelum ada peringkat
- Nutrients: Ultra-Processed Food Intake and Smoking Interact in Relation With Colorectal AdenomasDokumen15 halamanNutrients: Ultra-Processed Food Intake and Smoking Interact in Relation With Colorectal AdenomasAndrés Felipe Zapata MurielBelum ada peringkat
- 872 2540 2 PBDokumen4 halaman872 2540 2 PBSteve D'HamsBelum ada peringkat
- Downloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Dokumen28 halamanDownloaded From Uva-Dare, The Institutional Repository of The University of Amsterdam (Uva)Indah Putri permatasariBelum ada peringkat
- Bedah Digestif - Jurnal LaparotomiDokumen9 halamanBedah Digestif - Jurnal LaparotomiDenny EmiliusBelum ada peringkat
- Van Nella 2010Dokumen9 halamanVan Nella 2010Anonymous tSdibBveBelum ada peringkat
- 10 KotepuiDokumen5 halaman10 KotepuiAlfeus GradyBelum ada peringkat
- Epidemiologi KolestasisDokumen6 halamanEpidemiologi KolestasisDominikus Raditya AtmakaBelum ada peringkat
- Computacion 1Dokumen7 halamanComputacion 1lucas wiillianBelum ada peringkat
- Or3 PDFDokumen5 halamanOr3 PDFAkshay PatilBelum ada peringkat
- Admin,+3 +BHSJ+123+Angela+9-12+Vol+2 +no 1+2019Dokumen5 halamanAdmin,+3 +BHSJ+123+Angela+9-12+Vol+2 +no 1+2019Indra JayaBelum ada peringkat
- Iarjmsr 1 (3) 100-105Dokumen7 halamanIarjmsr 1 (3) 100-105jinuBelum ada peringkat
- HP Risc de Polip AdenomatosiDokumen5 halamanHP Risc de Polip AdenomatosiOctavian DumitruBelum ada peringkat
- Serosal Appendicitis: Incidence, Causes and Clinical SignificanceDokumen3 halamanSerosal Appendicitis: Incidence, Causes and Clinical SignificancenaufalrosarBelum ada peringkat
- International Incidence and Mortality Trends of Liver Cancer: A Global ProfileDokumen9 halamanInternational Incidence and Mortality Trends of Liver Cancer: A Global ProfileNovita ApramadhaBelum ada peringkat
- Jurnal 1Dokumen4 halamanJurnal 1TheQueensafa90Belum ada peringkat
- Rugge 2018Dokumen8 halamanRugge 2018Vanessa BecerraBelum ada peringkat
- Clinical Presentation and Treatment Outcomes of Thyroglossal Duct Cysts: A Systematic ReviewDokumen8 halamanClinical Presentation and Treatment Outcomes of Thyroglossal Duct Cysts: A Systematic ReviewR KBelum ada peringkat
- (International Journal of Cancer Vol. 77 Iss. 5) Milena Sant - Riccardo Capocaccia - Arduino Verdecchia - Jacques Es - Survival of Women With BreastDokumen5 halaman(International Journal of Cancer Vol. 77 Iss. 5) Milena Sant - Riccardo Capocaccia - Arduino Verdecchia - Jacques Es - Survival of Women With BreastTulioBelum ada peringkat
- Glycemic Control and Radiographic Manifestations of Tuberculosis in Diabetic PatientsDokumen17 halamanGlycemic Control and Radiographic Manifestations of Tuberculosis in Diabetic PatientsGlenda B AjilaBelum ada peringkat
- Urinary 1Dokumen7 halamanUrinary 1Yuni AstutiBelum ada peringkat
- KankerrrDokumen33 halamanKankerrrmey zizahBelum ada peringkat
- Genital and Urinary Tract Diseases and Bladder Cancer1Dokumen3 halamanGenital and Urinary Tract Diseases and Bladder Cancer1Okki Masitah Syahfitri NasutionBelum ada peringkat
- Processed MeatDokumen5 halamanProcessed MeatrobertBelum ada peringkat
- Clinical Study: Chronic Gastritis in Dermatitis Herpetiformis: A Controlled StudyDokumen5 halamanClinical Study: Chronic Gastritis in Dermatitis Herpetiformis: A Controlled Studyfirsa_artBelum ada peringkat
- Ari Cendani Prabawati (17.321.2658)Dokumen12 halamanAri Cendani Prabawati (17.321.2658)yuna pratiwiBelum ada peringkat
- Typhoid Perforation NepalDokumen3 halamanTyphoid Perforation NepalMagdalena PranataBelum ada peringkat
- Stevens JohsonDokumen8 halamanStevens JohsonDaily RomeroBelum ada peringkat
- CasAre There Risk Factors For Splenic Rupture During Colonoscopy CaseDokumen6 halamanCasAre There Risk Factors For Splenic Rupture During Colonoscopy Caseysh_girlBelum ada peringkat
- Overseas Screening For Tuberculosis in U.S.-Bound Immigrants and RefugeesDokumen10 halamanOverseas Screening For Tuberculosis in U.S.-Bound Immigrants and RefugeesprabuBelum ada peringkat
- Nutrition Management Ent FistDokumen11 halamanNutrition Management Ent FistyeyayoBelum ada peringkat
- Upper Tract Urothelial CarcinomaDari EverandUpper Tract Urothelial CarcinomaShahrokh F. ShariatBelum ada peringkat
- Money Tree International Finance Corp. Checklist of Standard Loan RequirementsDokumen2 halamanMoney Tree International Finance Corp. Checklist of Standard Loan RequirementsAgape LabuntogBelum ada peringkat
- Anti Stain Nsl30 Super - Msds - SdsDokumen8 halamanAnti Stain Nsl30 Super - Msds - SdsS.A. MohsinBelum ada peringkat
- Registration Statement (For Single Proprietor)Dokumen2 halamanRegistration Statement (For Single Proprietor)Sherwin SalanayBelum ada peringkat
- DPA Fact Sheet Women Prison and Drug War Jan2015 PDFDokumen2 halamanDPA Fact Sheet Women Prison and Drug War Jan2015 PDFwebmaster@drugpolicy.orgBelum ada peringkat
- Epicor Software India Private Limited: Brief Details of Your Form-16 Are As UnderDokumen9 halamanEpicor Software India Private Limited: Brief Details of Your Form-16 Are As UndersudhadkBelum ada peringkat
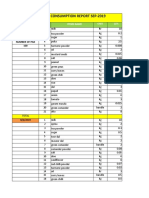
- Daily Staff Food Consumption Reports Sep-2019Dokumen4 halamanDaily Staff Food Consumption Reports Sep-2019Manjit RawatBelum ada peringkat
- Null 6 PDFDokumen1 halamanNull 6 PDFSimbarashe ChikariBelum ada peringkat
- Wisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseDokumen3 halamanWisconsin Humane Society To Acquire Kenosha's Safe Harbor Humane Society - Press ReleaseTMJ4 NewsBelum ada peringkat
- Minyak Atsiri Sereh WangiDokumen4 halamanMinyak Atsiri Sereh Wangicindy paraditha kasandraBelum ada peringkat
- Electrical Data: PD2310 ApplicationsDokumen1 halamanElectrical Data: PD2310 ApplicationsKSBelum ada peringkat
- Mycotoxin in Food Supply Chain (Peanuts)Dokumen2 halamanMycotoxin in Food Supply Chain (Peanuts)Ghanthimathi GvsBelum ada peringkat
- Principles of Health Management: Mokhlis Al Adham Pharmacist, MPHDokumen26 halamanPrinciples of Health Management: Mokhlis Al Adham Pharmacist, MPHYantoBelum ada peringkat
- Engineering Project ListDokumen25 halamanEngineering Project ListSyed ShaBelum ada peringkat
- Not Really A StoryDokumen209 halamanNot Really A StorySwapnaBelum ada peringkat
- Phardose Lab Prep 19 30Dokumen4 halamanPhardose Lab Prep 19 30POMPEYO BARROGABelum ada peringkat
- Answers To Your Questions About Circumcision and HIV/AIDSDokumen2 halamanAnswers To Your Questions About Circumcision and HIV/AIDSAlex BrownBelum ada peringkat
- Weld Metal Overlay & CladdingDokumen2 halamanWeld Metal Overlay & CladdingbobyBelum ada peringkat
- Congenital Flexural Deformity in CalfDokumen6 halamanCongenital Flexural Deformity in CalfBibek SutradharBelum ada peringkat
- Bisleri Water Industry: Project ReportDokumen53 halamanBisleri Water Industry: Project ReportJohn CarterBelum ada peringkat
- Rooftop Rain Water Harvesting in An Educational CampusDokumen9 halamanRooftop Rain Water Harvesting in An Educational CampusAkshay BoratiBelum ada peringkat
- 1A Wound Care AdviceDokumen2 halaman1A Wound Care AdviceGrace ValenciaBelum ada peringkat
- Chapter 2 Unfinished RRLDokumen22 halamanChapter 2 Unfinished RRLGM XylerBelum ada peringkat
- OPSS1213 Mar98Dokumen3 halamanOPSS1213 Mar98Tony ParkBelum ada peringkat