Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Helen Hodgson - Couple's Massage Handbook Deepen Your Relationship With The Healing Power of TouchDokumen268 halamanHelen Hodgson - Couple's Massage Handbook Deepen Your Relationship With The Healing Power of TouchLuca DatoBelum ada peringkat
- Emotional Intelligence Assignment 1 PDFDokumen10 halamanEmotional Intelligence Assignment 1 PDFAbdelßasset Zkr100% (2)
- ToonHub - Articles of PartnershipDokumen13 halamanToonHub - Articles of PartnershipKingBelum ada peringkat
- Grade 2 - PAN-ASSESSMENT-TOOLDokumen5 halamanGrade 2 - PAN-ASSESSMENT-TOOLMaestro Varix100% (4)
- ! Sco Global Impex 25.06.20Dokumen7 halaman! Sco Global Impex 25.06.20Houssam Eddine MimouneBelum ada peringkat
- Cookery-10 LAS-Q3 Week5Dokumen7 halamanCookery-10 LAS-Q3 Week5Angeline Cortez100% (1)
- Leadership Style and Employee Turnover IntentionsDokumen21 halamanLeadership Style and Employee Turnover IntentionsAbdelßasset ZkrBelum ada peringkat
- Ijias 15 262 04Dokumen5 halamanIjias 15 262 04Abdelßasset ZkrBelum ada peringkat
- 2Dokumen6 halaman2Abdelßasset ZkrBelum ada peringkat
- Why Management Skills Are A Priority For Nurses 050313Dokumen2 halamanWhy Management Skills Are A Priority For Nurses 050313Rauven Jean Erodias FadriquelaBelum ada peringkat
- Emotional IntelligenceDokumen3 halamanEmotional IntelligenceAbdelßasset ZkrBelum ada peringkat
- Dietery Factor Obesity Microenvironnement and Breast CancerDokumen9 halamanDietery Factor Obesity Microenvironnement and Breast CancerAbdelßasset ZkrBelum ada peringkat
- Knowledge, Attitudes and Practices Toward Breast CancerDokumen9 halamanKnowledge, Attitudes and Practices Toward Breast CancerAbdelßasset ZkrBelum ada peringkat
- A Beautiful MindDokumen6 halamanA Beautiful MindAbdelßasset ZkrBelum ada peringkat
- The Relationship of Turnover Intention With Job Satisfaction, Job Performance, Leader Member Exchange, Emotional Intelligence and Organizational CommitmentDokumen15 halamanThe Relationship of Turnover Intention With Job Satisfaction, Job Performance, Leader Member Exchange, Emotional Intelligence and Organizational CommitmentgaluhfitriBelum ada peringkat
- Emotional IntelligenceDokumen3 halamanEmotional IntelligenceAbdelßasset ZkrBelum ada peringkat
- EQ Interview Assignment - Evaluate Candidate's Empathy SkillsDokumen1 halamanEQ Interview Assignment - Evaluate Candidate's Empathy SkillsAbdelßasset ZkrBelum ada peringkat
- Why Management Skills Are A Priority For Nurses 050313Dokumen2 halamanWhy Management Skills Are A Priority For Nurses 050313Rauven Jean Erodias FadriquelaBelum ada peringkat
- FIITJEE Talent Reward Exam 2020: Proctored Online Test - Guidelines For StudentsDokumen3 halamanFIITJEE Talent Reward Exam 2020: Proctored Online Test - Guidelines For StudentsShivesh PANDEYBelum ada peringkat
- Unofficial Transcript - Printer FriendlyDokumen4 halamanUnofficial Transcript - Printer Friendlyapi-251794642Belum ada peringkat
- Research Methods LessonDokumen26 halamanResearch Methods LessonCarole Janne EndoyBelum ada peringkat
- Specification Table - Stocks and ETF CFDsDokumen53 halamanSpecification Table - Stocks and ETF CFDsHouse GardenBelum ada peringkat
- Other Project Content-1 To 8Dokumen8 halamanOther Project Content-1 To 8Amit PasiBelum ada peringkat
- Bhikkhuni Patimokkha Fourth Edition - Pali and English - UTBSI Ordination Bodhgaya Nov 2022 (E-Book Version)Dokumen154 halamanBhikkhuni Patimokkha Fourth Edition - Pali and English - UTBSI Ordination Bodhgaya Nov 2022 (E-Book Version)Ven. Tathālokā TherīBelum ada peringkat
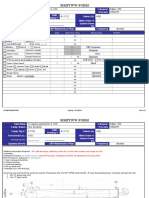
- Simptww S-1105Dokumen3 halamanSimptww S-1105Vijay RajaindranBelum ada peringkat
- Dealer DirectoryDokumen83 halamanDealer DirectorySportivoBelum ada peringkat
- Term2 WS7 Revision2 PDFDokumen5 halamanTerm2 WS7 Revision2 PDFrekhaBelum ada peringkat
- Robots Template 16x9Dokumen13 halamanRobots Template 16x9Danika Kaye GornesBelum ada peringkat
- CV Finance GraduateDokumen3 halamanCV Finance GraduateKhalid SalimBelum ada peringkat
- Dues & Scholarship Section: NotificationDokumen6 halamanDues & Scholarship Section: NotificationMUNEEB WAHEEDBelum ada peringkat
- MES - Project Orientation For Night Study - V4Dokumen41 halamanMES - Project Orientation For Night Study - V4Andi YusmarBelum ada peringkat
- License Key Windows 8Dokumen7 halamanLicense Key Windows 8Juned FahriBelum ada peringkat
- Das MarterkapitalDokumen22 halamanDas MarterkapitalMatthew Shen GoodmanBelum ada peringkat
- Diabetic Foot InfectionDokumen26 halamanDiabetic Foot InfectionAmanda Abdat100% (1)
- Sustainable Marketing and Consumers Preferences in Tourism 2167Dokumen5 halamanSustainable Marketing and Consumers Preferences in Tourism 2167DanielBelum ada peringkat
- FOL Predicate LogicDokumen23 halamanFOL Predicate LogicDaniel Bido RasaBelum ada peringkat
- Lucid Motors Stock Prediction 2022, 2023, 2024, 2025, 2030Dokumen8 halamanLucid Motors Stock Prediction 2022, 2023, 2024, 2025, 2030Sahil DadashovBelum ada peringkat
- 100 Bedded Hospital at Jadcherla: Load CalculationsDokumen3 halaman100 Bedded Hospital at Jadcherla: Load Calculationskiran raghukiranBelum ada peringkat
- Statement of Purpose EitDokumen3 halamanStatement of Purpose EitSajith KvBelum ada peringkat
- TOPIC - 1 - Intro To Tourism PDFDokumen16 halamanTOPIC - 1 - Intro To Tourism PDFdevvy anneBelum ada peringkat
- PAASCU Lesson PlanDokumen2 halamanPAASCU Lesson PlanAnonymous On831wJKlsBelum ada peringkat
- Ten Lessons (Not?) Learnt: Asset AllocationDokumen30 halamanTen Lessons (Not?) Learnt: Asset AllocationkollingmBelum ada peringkat
- MAS-06 WORKING CAPITAL OPTIMIZATIONDokumen9 halamanMAS-06 WORKING CAPITAL OPTIMIZATIONEinstein Salcedo100% (1)