Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Real Estate Developer Resume SampleDokumen1 halamanReal Estate Developer Resume Sampleresume7.com100% (2)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Corephotonics Dual-Camera LawsuitDokumen53 halamanCorephotonics Dual-Camera LawsuitMikey CampbellBelum ada peringkat
- Zaranda Finlay 684 Manual Parts CatalogDokumen405 halamanZaranda Finlay 684 Manual Parts CatalogRicky Vil100% (2)
- Embedded CoderDokumen8 halamanEmbedded Coderجمال طيبيBelum ada peringkat
- Instrumen PKPO SNARS 1.1Dokumen33 halamanInstrumen PKPO SNARS 1.1Achmad FachryBelum ada peringkat
- Food Drug InteractionDokumen32 halamanFood Drug InteractionAchmad FachryBelum ada peringkat
- Instrumen MIRM Ed 1.1Dokumen27 halamanInstrumen MIRM Ed 1.1Achmad FachryBelum ada peringkat
- Ajay Bhalla, Jonathan Birns (Eds.) - Management of Post-Stroke Complications-Springer International Publishing (2015) PDFDokumen393 halamanAjay Bhalla, Jonathan Birns (Eds.) - Management of Post-Stroke Complications-Springer International Publishing (2015) PDFAchmad FachryBelum ada peringkat
- Chlorpheniramine MaleatDokumen200 halamanChlorpheniramine MaleatAchmad Fachry100% (1)
- Fmea 2016Dokumen96 halamanFmea 2016tami lestariBelum ada peringkat
- Jonathan Sudharta e - PrescriptionDokumen53 halamanJonathan Sudharta e - PrescriptionAchmad FachryBelum ada peringkat
- Fmea 2016Dokumen96 halamanFmea 2016tami lestariBelum ada peringkat
- Theraputics JournalDokumen88 halamanTheraputics JournalAchmad FachryBelum ada peringkat
- Nevirapine: Indications CautionsDokumen3 halamanNevirapine: Indications CautionsAchmad FachryBelum ada peringkat
- Tot - Terapi Arv (4s)Dokumen66 halamanTot - Terapi Arv (4s)Farkhana MmdBelum ada peringkat
- Drug Absorption PDFDokumen117 halamanDrug Absorption PDFAndhia DhiyaBelum ada peringkat
- Drug Absorption PDFDokumen117 halamanDrug Absorption PDFAndhia DhiyaBelum ada peringkat
- Pharmaceutical Care Case StudiesDokumen4 halamanPharmaceutical Care Case StudiesAchmad FachryBelum ada peringkat
- MedicineDokumen53 halamanMedicineapi-25984682100% (1)
- Clinical Trials Handbook TGADokumen36 halamanClinical Trials Handbook TGAxarghyaBelum ada peringkat
- Screenshot 2021-10-02 at 12.22.29 PMDokumen1 halamanScreenshot 2021-10-02 at 12.22.29 PMSimran SainiBelum ada peringkat
- Lunakleen: Standard Type Hepa FilterDokumen1 halamanLunakleen: Standard Type Hepa FilterRyan Au YongBelum ada peringkat
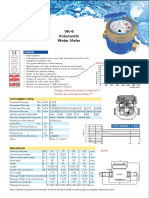
- Baylan: VK-6 Volumetric Water MeterDokumen1 halamanBaylan: VK-6 Volumetric Water MeterSanjeewa ChathurangaBelum ada peringkat
- This Study Resource Was: ExercisesDokumen1 halamanThis Study Resource Was: Exercisesىوسوكي صانتوسBelum ada peringkat
- Encore HR PresentationDokumen8 halamanEncore HR PresentationLatika MalhotraBelum ada peringkat
- Detect Single-Phase Issues with Negative Sequence RelayDokumen7 halamanDetect Single-Phase Issues with Negative Sequence RelayluhusapaBelum ada peringkat
- FINAL Session 3 Specific GuidelinesDokumen54 halamanFINAL Session 3 Specific GuidelinesBovelyn Autida-masingBelum ada peringkat
- NPTEL Web Course On Complex Analysis: A. SwaminathanDokumen19 halamanNPTEL Web Course On Complex Analysis: A. SwaminathanMohit SharmaBelum ada peringkat
- CEMEX Global Strategy CaseDokumen4 halamanCEMEX Global Strategy CaseSaif Ul Islam100% (1)
- Kinds of ObligationDokumen50 halamanKinds of ObligationKIM GABRIEL PAMITTANBelum ada peringkat
- Ibad Rehman CV NewDokumen4 halamanIbad Rehman CV NewAnonymous ECcVsLBelum ada peringkat
- National Income Practice QuestionsDokumen29 halamanNational Income Practice QuestionsSujalBelum ada peringkat
- HOS Dials in The Driver App - Samsara SupportDokumen3 halamanHOS Dials in The Driver App - Samsara SupportMaryBelum ada peringkat
- Igbt Irg 4p254sDokumen9 halamanIgbt Irg 4p254sMilagros Mendieta VegaBelum ada peringkat
- Chapter 2 FlywheelDokumen24 halamanChapter 2 Flywheelshazwani zamriBelum ada peringkat
- Sahrudaya Health Care Private Limited: Pay Slip For The Month of May-2022Dokumen1 halamanSahrudaya Health Care Private Limited: Pay Slip For The Month of May-2022Rohit raagBelum ada peringkat
- Loans and AdvanceDokumen8 halamanLoans and AdvanceDjay SlyBelum ada peringkat
- Secure Access Control and Browser Isolation PrinciplesDokumen32 halamanSecure Access Control and Browser Isolation PrinciplesSushant Yadav100% (1)
- Mosfet PDFDokumen13 halamanMosfet PDFTad-electronics TadelectronicsBelum ada peringkat
- Danielle Smith: To Whom It May ConcernDokumen2 halamanDanielle Smith: To Whom It May ConcernDanielle SmithBelum ada peringkat
- 22 Caltex Philippines, Inc. vs. Commission On Audit, 208 SCRA 726, May 08, 1992Dokumen36 halaman22 Caltex Philippines, Inc. vs. Commission On Audit, 208 SCRA 726, May 08, 1992milkteaBelum ada peringkat
- Delem: Installation Manual V3Dokumen73 halamanDelem: Installation Manual V3Marcus ChuaBelum ada peringkat
- Lessee Information StatementDokumen1 halamanLessee Information Statementmja.carilloBelum ada peringkat
- Example Italy ItenararyDokumen35 halamanExample Italy ItenararyHafshary D. ThanialBelum ada peringkat
- Converted File d7206cc0Dokumen15 halamanConverted File d7206cc0warzarwBelum ada peringkat
- Readiness of Barangay Masalukot During TyphoonsDokumen34 halamanReadiness of Barangay Masalukot During TyphoonsJerome AbrigoBelum ada peringkat