Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Practice: Diagnosis and Management of Gallstone Disease: Summary of NICE GuidanceDokumen3 halamanPractice: Diagnosis and Management of Gallstone Disease: Summary of NICE GuidanceKoas PatoBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Clinical Presentations and Outcome of Severe Community-Acquired PneumoniaDokumen9 halamanClinical Presentations and Outcome of Severe Community-Acquired PneumoniaKoas PatoBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Mola Hidatidosa1 PDFDokumen8 halamanMola Hidatidosa1 PDFKoas PatoBelum ada peringkat
- Journal DermatologyDokumen3 halamanJournal DermatologyKoas PatoBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- PubMed7 PDFDokumen15 halamanPubMed7 PDFKoas PatoBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Journal DermatologyDokumen4 halamanJournal DermatologyKoas PatoBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Psoriasis of The Face and FlexuresDokumen10 halamanPsoriasis of The Face and FlexuresKoas PatoBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Otitis EksternaDokumen9 halamanOtitis EksternaKoas PatoBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Dermatology JournalDokumen8 halamanDermatology JournalKoas PatoBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Dermatology JournalDokumen17 halamanDermatology JournalKoas PatoBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Acn30001 0171 PDFDokumen9 halamanAcn30001 0171 PDFKoas PatoBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Level 9 - Unit 34Dokumen7 halamanLevel 9 - Unit 34Javier RiquelmeBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- 03 - Air Ticket Request & Claim Form 2018Dokumen1 halaman03 - Air Ticket Request & Claim Form 2018Danny SolvanBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Materials Management in Hospital Industry Nandi ProjectDokumen27 halamanMaterials Management in Hospital Industry Nandi Projectkumaraswamy226Belum ada peringkat
- Wax Depilation ManualDokumen17 halamanWax Depilation ManualAmit Sharma100% (1)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Republic Act No. 10070Dokumen3 halamanRepublic Act No. 10070Ganiela MCBelum ada peringkat
- Interview Questionaries (Cont.)Dokumen27 halamanInterview Questionaries (Cont.)shubha christopherBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Random FactsDokumen353 halamanRandom FactsSergio Rivas100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- 01 Mono Channel BurnerDokumen1 halaman01 Mono Channel BurnerSelwyn MunatsiBelum ada peringkat
- PCB Engraver Operator Manual PDFDokumen41 halamanPCB Engraver Operator Manual PDFmyoshkeuBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Strep Throat FactsDokumen2 halamanStrep Throat FactsFactPaloozaBelum ada peringkat
- EC Type-Examination Certificate: Reg.-No.: 01/205/5192.02/18Dokumen11 halamanEC Type-Examination Certificate: Reg.-No.: 01/205/5192.02/18Orlando Ortiz VillegasBelum ada peringkat
- Case Analysis of Vishal Jeet V. Union of India Trafficking of Women and ChildrenDokumen7 halamanCase Analysis of Vishal Jeet V. Union of India Trafficking of Women and ChildrenTrishani NahaBelum ada peringkat
- PACKET 1 - Exercises and ActivitiesDokumen7 halamanPACKET 1 - Exercises and ActivitiesPrantsir Pernes100% (2)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Green Partnership of The Future: DieselfactsDokumen12 halamanGreen Partnership of The Future: DieselfactsKamal WanniarachchiBelum ada peringkat
- Pakistan Hse Requirements and Guidlines For Drilling OperationsDokumen52 halamanPakistan Hse Requirements and Guidlines For Drilling OperationstyoBelum ada peringkat
- Writing Workshop G7 PDFDokumen12 halamanWriting Workshop G7 PDFJobell AguvidaBelum ada peringkat
- Water Quantity Estimation PDFDokumen3 halamanWater Quantity Estimation PDFOladunni AfolabiBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Adjectives Comparative and Superlative FormDokumen5 halamanAdjectives Comparative and Superlative FormOrlando MiguelBelum ada peringkat
- TG Chap. 10Dokumen7 halamanTG Chap. 10Gissele AbolucionBelum ada peringkat
- ProjectxDokumen8 halamanProjectxAvinash KumarBelum ada peringkat
- CSF LeaksDokumen3 halamanCSF LeaksDrTarek Mahmoud Abo KammerBelum ada peringkat
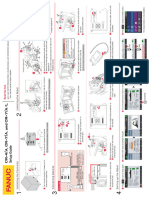
- CR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)Dokumen1 halamanCR-7iA CR-4iA Installation and Setup Guide (B-83774JA-1 01)lidiia.pavlkukBelum ada peringkat
- Accomplishment Report Rle Oct.Dokumen7 halamanAccomplishment Report Rle Oct.krull243Belum ada peringkat
- Gpat Reference NotesDokumen9 halamanGpat Reference NotesPreethi KiranBelum ada peringkat
- Akin To PityDokumen356 halamanAkin To PityPaul StewartBelum ada peringkat
- Emissivity Table E4Dokumen11 halamanEmissivity Table E4Mekro Permana PinemBelum ada peringkat
- Molecular MechanicsDokumen26 halamanMolecular MechanicsKarthi ShanmugamBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- LIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyDokumen2 halamanLIST OF REGISTERED DRUGS As of December 2012: DR No Generic Brand Strength Form CompanyBenjamin TantiansuBelum ada peringkat
- Rekapan Belanja JKNDokumen5 halamanRekapan Belanja JKNAPOTEK PUSKESMAS MALEBERBelum ada peringkat
- O OP PE ER RA Attiin NG G Iin NS STTR RU UC Cttiio ON NS S: UF 755 G UF 455 GDokumen14 halamanO OP PE ER RA Attiin NG G Iin NS STTR RU UC Cttiio ON NS S: UF 755 G UF 455 GHomeroPerezBelum ada peringkat