Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- A Holistic Approach To AutismDokumen11 halamanA Holistic Approach To AutismNapoleon Gonzalez Gil100% (2)
- Buttler, Irene Dr. Thornton, Karen 17851920Dokumen1 halamanButtler, Irene Dr. Thornton, Karen 17851920ahmedBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Molecular Virology, 2013 Edition (PDF) (DR - Carson) VRG PDFDokumen1.013 halamanMolecular Virology, 2013 Edition (PDF) (DR - Carson) VRG PDFYuridia Rodríguez100% (3)
- Michael S. Niederman Severe Pneumonia Lung Biology in Health and Disease, Volume 206Dokumen450 halamanMichael S. Niederman Severe Pneumonia Lung Biology in Health and Disease, Volume 206Alirio Bastidas0% (1)
- Yr 10 Revision BookletDokumen41 halamanYr 10 Revision Bookletdeepheat_008100% (1)
- Mpeh Grade8 Pre-TestDokumen3 halamanMpeh Grade8 Pre-TestElmie Valencia-Cuachon77% (53)
- pathoPHYSIOLOGY OF OSTEOMYELITIS (DIAGRAM)Dokumen1 halamanpathoPHYSIOLOGY OF OSTEOMYELITIS (DIAGRAM)redhoney100% (5)
- InfeccionDokumen3 halamanInfeccionJoao Alcca Benites100% (1)
- Impact of Covid-19 in Our SocietyDokumen25 halamanImpact of Covid-19 in Our SocietyAISHA 20682Belum ada peringkat
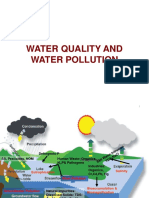
- 3 Water QualityDokumen98 halaman3 Water QualityPraveen KumarBelum ada peringkat
- Primary Health CareDokumen133 halamanPrimary Health CareSteveBelum ada peringkat
- Listeria MonocytogenesDokumen28 halamanListeria Monocytogenestummalapalli venkateswara rao100% (1)
- Urinary Tract InfectionsDokumen44 halamanUrinary Tract Infectionstummalapalli venkateswara rao100% (2)
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Dokumen13 halamanP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Rofa Husnul KhuluqiBelum ada peringkat
- Responsi by RofaDokumen19 halamanResponsi by RofaRofa Husnul KhuluqiBelum ada peringkat
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Dokumen9 halamanP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Rofa Husnul KhuluqiBelum ada peringkat
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Dokumen13 halamanP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Rofa Husnul KhuluqiBelum ada peringkat
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Dokumen11 halamanP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Rofa Husnul KhuluqiBelum ada peringkat
- G.S V LeeDokumen29 halamanG.S V LeeDan LehrBelum ada peringkat
- Ch04oral MedicineDokumen35 halamanCh04oral MedicineNaleena JosephBelum ada peringkat
- Chronic Lung Transplant Rejection - Bronchiolitis Obliterans - UpToDateDokumen36 halamanChronic Lung Transplant Rejection - Bronchiolitis Obliterans - UpToDatemihaela popescuBelum ada peringkat
- At The End of The Lesson, The Learners Should Be Able ToDokumen4 halamanAt The End of The Lesson, The Learners Should Be Able ToHarold Nalla HusayanBelum ada peringkat
- Nursing Care Plan For Client With Risk of InfectionDokumen2 halamanNursing Care Plan For Client With Risk of InfectionThe Right WayBelum ada peringkat
- Multilaboratory Assessment of Metagenomic Next-Generation Sequencing For Unbiased Microbe DetectionDokumen10 halamanMultilaboratory Assessment of Metagenomic Next-Generation Sequencing For Unbiased Microbe DetectionIndriani BaharuddinBelum ada peringkat
- A MatrixDokumen11 halamanA MatrixChristian MakandeBelum ada peringkat
- Fergusson College (Autonomous) Pune: MicrobiologyDokumen15 halamanFergusson College (Autonomous) Pune: MicrobiologyAAABelum ada peringkat
- Torres 7TH EditionDokumen67 halamanTorres 7TH EditionDrexel DalaygonBelum ada peringkat
- Bat CoronavirusesDokumen15 halamanBat CoronavirusesRITURAJ ACHARYABelum ada peringkat
- An Immunochromatographic Test Strip For Rapid Detection of Fish Pathogen Edwardsiella TardaDokumen8 halamanAn Immunochromatographic Test Strip For Rapid Detection of Fish Pathogen Edwardsiella Tardagershom mbwamboBelum ada peringkat
- OKU Musculo Infection CH 04Dokumen12 halamanOKU Musculo Infection CH 04Jose Enrique FonsecaBelum ada peringkat
- Journal of Infection: Letter To The EditorDokumen4 halamanJournal of Infection: Letter To The EditorAli AlaviBelum ada peringkat
- Why Do We Fall IllDokumen8 halamanWhy Do We Fall IllSukhda TrivediBelum ada peringkat
- Tetracycline SDokumen51 halamanTetracycline SPapaindoBelum ada peringkat
- Demography: Sources of Demographic DataDokumen8 halamanDemography: Sources of Demographic DataSHERMINA HASANBelum ada peringkat
- 2nd SHIFTING EXAM Schedule and CoverageDokumen2 halaman2nd SHIFTING EXAM Schedule and CoverageEliza Paula BacudBelum ada peringkat