Anda mungkin juga menyukai
- Liver Imaging: MRI with CT CorrelationDari EverandLiver Imaging: MRI with CT CorrelationErsan AltunBelum ada peringkat
- CSF Flowmetry MriDokumen5 halamanCSF Flowmetry MribricklaneBelum ada peringkat
- Atlas of Surgical Pathology GrossingDari EverandAtlas of Surgical Pathology GrossingMonica B. LemosBelum ada peringkat
- Liquor CerebrospinalisDokumen25 halamanLiquor CerebrospinalisIhda ParidahBelum ada peringkat
- Women's Imaging: MRI with Multimodality CorrelationDari EverandWomen's Imaging: MRI with Multimodality CorrelationMichele A. BrownPenilaian: 5 dari 5 bintang5/5 (1)
- BILIARY TRACT DISEASE: GALLSTONES, CHOLECYSTITIS, CHOLEDOCHOLITHIASIS, AND CHOLANGITISDokumen6 halamanBILIARY TRACT DISEASE: GALLSTONES, CHOLECYSTITIS, CHOLEDOCHOLITHIASIS, AND CHOLANGITISRafael KameradBelum ada peringkat
- X-Ray Reveals Skull Lesions in Multiple Myeloma PatientDokumen63 halamanX-Ray Reveals Skull Lesions in Multiple Myeloma Patient李建明Belum ada peringkat
- Brain Ventricles AnatomyDokumen25 halamanBrain Ventricles AnatomyMiazan SheikhBelum ada peringkat
- Liver EcoDokumen40 halamanLiver EcoGelu Rad100% (1)
- Molar Pregnancy PDFDokumen8 halamanMolar Pregnancy PDFEgaSuharnoBelum ada peringkat
- Retrohepatic Gallbladder Masquerading As Hydatid Cyst in ADokumen18 halamanRetrohepatic Gallbladder Masquerading As Hydatid Cyst in AMadalina BlagaBelum ada peringkat
- Radiology Techniques & Processes GuideDokumen27 halamanRadiology Techniques & Processes GuideHarmas Novryan FarezaBelum ada peringkat
- The Normal CSFDokumen2 halamanThe Normal CSFUm MahmoudBelum ada peringkat
- Unit 5 Medical UltrasoundDokumen6 halamanUnit 5 Medical Ultrasoundtwy113Belum ada peringkat
- Lower Limb Radiology GuideDokumen65 halamanLower Limb Radiology GuideVivien EnriquezBelum ada peringkat
- Cerebrospinal Liquor and Its CirculationDokumen13 halamanCerebrospinal Liquor and Its CirculationusergrBelum ada peringkat
- Classical Radiological SignsDokumen2 halamanClassical Radiological SignsMuntaha JavedBelum ada peringkat
- Doppler of Varicose VeinsDokumen85 halamanDoppler of Varicose VeinsDiaa Eldeeb100% (2)
- CT Brain Part II-AnatomyDokumen65 halamanCT Brain Part II-AnatomyXhenni XhenniBelum ada peringkat
- IVUS PresentationDokumen32 halamanIVUS PresentationSam ExlerBelum ada peringkat
- IVUS Image GuideDokumen17 halamanIVUS Image GuideRajesh JayakumarBelum ada peringkat
- Clinical Imaging of Liver, Gallbladder, BiliaryDokumen93 halamanClinical Imaging of Liver, Gallbladder, Biliaryapi-3856051100% (1)
- Ardms Spi Exam.pdfDokumen336 halamanArdms Spi Exam.pdfSanjida PiyaBelum ada peringkat
- Interventional Radiology & AngiographyDokumen45 halamanInterventional Radiology & AngiographyRyBone95Belum ada peringkat
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDokumen26 halamanAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailBelum ada peringkat
- Ultrasound: Made By: Conny LeoDokumen15 halamanUltrasound: Made By: Conny LeoChristabelle ConnyBelum ada peringkat
- DR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & Imaging BsmmuDokumen46 halamanDR - Shamim Rima MBBS, Dmu, FCGP M.Phil Radiology & Imaging Bsmmudr_shamimr100% (1)
- Echocardiographic Assessment of Valve Stenosis: Heart Circulation Ultrasound SpecialistsDokumen1 halamanEchocardiographic Assessment of Valve Stenosis: Heart Circulation Ultrasound SpecialistsWayan GunawanBelum ada peringkat
- How Can I Distinguish Myself On Clinical RotationsDokumen2 halamanHow Can I Distinguish Myself On Clinical Rotationspatricka13Belum ada peringkat
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDokumen42 halamanHepatobiliary Disorders: Katrina Saludar Jimenez, R. NreykatBelum ada peringkat
- Ultrasonography of The Hepatobiliary TractDokumen9 halamanUltrasonography of The Hepatobiliary TractPaola Méndez NeciosupBelum ada peringkat
- Vascular Disorders StudentsDokumen70 halamanVascular Disorders StudentsedwinBelum ada peringkat
- Infertile Couple - Role of Ultrasound FinalDokumen31 halamanInfertile Couple - Role of Ultrasound FinalKalpavriksha1974Belum ada peringkat
- Doppler Ultrasonography of The Lower Extremity ArteriesDokumen34 halamanDoppler Ultrasonography of The Lower Extremity ArteriesNidaa MubarakBelum ada peringkat
- Participate in Board Questions: Ascexam / ReasceDokumen105 halamanParticipate in Board Questions: Ascexam / ReasceSharma RomeoBelum ada peringkat
- Cardiology: Anatomy of the Heart and MediastinumDokumen13 halamanCardiology: Anatomy of the Heart and MediastinumJennifer SteffiBelum ada peringkat
- AnatomyDokumen94 halamanAnatomypshahBelum ada peringkat
- Lumber Spine and Pelvis RadiographyDokumen84 halamanLumber Spine and Pelvis RadiographyMunish DograBelum ada peringkat
- Brachial PlexusDokumen9 halamanBrachial PlexusKhadeeja NaqviBelum ada peringkat
- Simple Office SpirometryDokumen42 halamanSimple Office SpirometryRoberto Merza III100% (4)
- CSF and Cerebral Blood FlowDokumen58 halamanCSF and Cerebral Blood FlowCindy PrayogoBelum ada peringkat
- Liver: Presented by Dr. Tahmina Islam MD Third PartDokumen121 halamanLiver: Presented by Dr. Tahmina Islam MD Third PartNajib JamilBelum ada peringkat
- Ultrasound Și DopplerDokumen3 halamanUltrasound Și DopplerAurelia AlexandraBelum ada peringkat
- Blood Can Be Very BadDokumen37 halamanBlood Can Be Very BadPhil SingerBelum ada peringkat
- Septum Formation in The VentriclesDokumen43 halamanSeptum Formation in The VentriclesAhsan IslamBelum ada peringkat
- DR Kaushal Cerebral Blood FlowDokumen52 halamanDR Kaushal Cerebral Blood Flowoddie333Belum ada peringkat
- Pediatric Echocardiography: Understanding Congenital Heart DefectsDokumen159 halamanPediatric Echocardiography: Understanding Congenital Heart DefectsSergiu NiculitaBelum ada peringkat
- Chest X-RayDokumen101 halamanChest X-RayYuke04Belum ada peringkat
- IMD - Step-Up To USMLE Step 3 - Chapter 1 - CardiologyDokumen124 halamanIMD - Step-Up To USMLE Step 3 - Chapter 1 - CardiologyAly SherifBelum ada peringkat
- Bosniak ClassificationDokumen19 halamanBosniak ClassificationGirish Kumar100% (1)
- Imaging in Abdominal TraumaDokumen133 halamanImaging in Abdominal TraumaEdward Arthur IskandarBelum ada peringkat
- Doppler Ultrasound: Understanding the Doppler Effect, Modes, and TerminologyDokumen54 halamanDoppler Ultrasound: Understanding the Doppler Effect, Modes, and TerminologyattooBelum ada peringkat
- Imaging of The Respiratory SystemDokumen105 halamanImaging of The Respiratory SystemMizrab Nadeem100% (1)
- Clinical Radiology Subspecialty Web Review of GI ResourcesDokumen3 halamanClinical Radiology Subspecialty Web Review of GI Resourcesarsalanraza1978Belum ada peringkat
- P1Dokumen12 halamanP1Roykedona Lisa TrixieBelum ada peringkat
- Reading A Head CT, What Every EP Should Know PDFDokumen62 halamanReading A Head CT, What Every EP Should Know PDFAdistya Sari100% (1)
- CT ScanDokumen12 halamanCT ScanNita ThrenitatiaBelum ada peringkat
- Interpretasi CT ScanDokumen19 halamanInterpretasi CT ScanAB KristiadiBelum ada peringkat
- San 12193Dokumen6 halamanSan 12193Karla BFBelum ada peringkat
- CT Brain Findings in ER PatientsDokumen84 halamanCT Brain Findings in ER PatientsAbegail IbañezBelum ada peringkat
- Wereldleiders Op TwitterDokumen24 halamanWereldleiders Op TwitterHerman CouwenberghBelum ada peringkat
- TRAI Data Till 31st March, 2014Dokumen19 halamanTRAI Data Till 31st March, 2014Tamanna Bavishi ShahBelum ada peringkat
- NokiaDokumen1 halamanNokiaSumit RoyBelum ada peringkat
- The State of Mobile Advertising in Emerging Countries TLS EmergingMarketsDokumen8 halamanThe State of Mobile Advertising in Emerging Countries TLS EmergingMarketsSumit RoyBelum ada peringkat
- Risk Factors From Hepatitis BCDDokumen1 halamanRisk Factors From Hepatitis BCDSumit RoyBelum ada peringkat
- Mobile Advertising Research Trends and InsightsDokumen15 halamanMobile Advertising Research Trends and InsightsSumit RoyBelum ada peringkat
- Hepatitis A eDokumen1 halamanHepatitis A eSumit RoyBelum ada peringkat
- Nightingales - Philips Healthcare Tie UpDokumen3 halamanNightingales - Philips Healthcare Tie UpSumit RoyBelum ada peringkat
- World Health Days 2014: JanuaryDokumen2 halamanWorld Health Days 2014: JanuaryIvy Jorene Roman RodriguezBelum ada peringkat
- Hepatitis A eDokumen1 halamanHepatitis A eSumit RoyBelum ada peringkat
- The State of Airline Marketing Airlinetrends Simpliflying April2013Dokumen21 halamanThe State of Airline Marketing Airlinetrends Simpliflying April2013Sumit RoyBelum ada peringkat
- Calendário de Jogos Do Mundial de Futebol-Brasil 2014Dokumen0 halamanCalendário de Jogos Do Mundial de Futebol-Brasil 2014Miguel RodriguesBelum ada peringkat
- FINAL - Mobile Advertising DeckDokumen73 halamanFINAL - Mobile Advertising DecksumitkroyBelum ada peringkat
- Global Top 100 Most Valueable Brands Brandz2014 - Infographic PDFDokumen1 halamanGlobal Top 100 Most Valueable Brands Brandz2014 - Infographic PDFSumit RoyBelum ada peringkat
- The State of Maternal Health, D Nutrition in Asia " World Vision DataDokumen4 halamanThe State of Maternal Health, D Nutrition in Asia " World Vision DataSumit RoyBelum ada peringkat
- World Health Statisitics FullDokumen180 halamanWorld Health Statisitics FullClarice SalidoBelum ada peringkat
- Calendar 14Dokumen57 halamanCalendar 14Hanan AhmedBelum ada peringkat
- Mediamind Comscore Research Dwelling On EntertainmentDokumen20 halamanMediamind Comscore Research Dwelling On EntertainmentSumit RoyBelum ada peringkat
- MGI China E-Tailing Executive Summary March 2013Dokumen18 halamanMGI China E-Tailing Executive Summary March 2013Sumit RoyBelum ada peringkat
- The 5 Free Alternatives To Microsoft WordDokumen60 halamanThe 5 Free Alternatives To Microsoft WordSumit RoyBelum ada peringkat
- CEO Survey On Hiring, Profitability and PeopleDokumen36 halamanCEO Survey On Hiring, Profitability and PeopleSumit RoyBelum ada peringkat
- The Evolution of Digital Advertising 3.0: Adobe Research InsightsDokumen1 halamanThe Evolution of Digital Advertising 3.0: Adobe Research InsightsSumit RoyBelum ada peringkat
- The 5 Free Alternatives To Microsoft WordDokumen60 halamanThe 5 Free Alternatives To Microsoft WordSumit RoyBelum ada peringkat
- 2014 Bill and Melinda Gates Foundation Report On Global PovertyDokumen28 halaman2014 Bill and Melinda Gates Foundation Report On Global PovertySumit RoyBelum ada peringkat
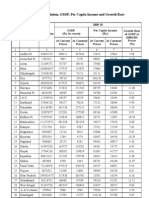
- Statewise GSDP PCI and G.RDokumen3 halamanStatewise GSDP PCI and G.RArchit SingalBelum ada peringkat
- 10 Historical Speeches Nobody Ever HeardDokumen20 halaman10 Historical Speeches Nobody Ever HeardSumit Roy100% (1)
- Gender and Social Networking Activity :facebook Vs OthersDokumen18 halamanGender and Social Networking Activity :facebook Vs OthersSumit RoyBelum ada peringkat
- CVD Atlas 16 Death From Stroke PDFDokumen1 halamanCVD Atlas 16 Death From Stroke PDFRisti KhafidahBelum ada peringkat
- India InfographicsDokumen3 halamanIndia InfographicsSumit RoyBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBelum ada peringkat
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementDari EverandTechniques Exercises And Tricks For Memory ImprovementPenilaian: 4.5 dari 5 bintang4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsPenilaian: 5 dari 5 bintang5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 5 dari 5 bintang5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesDari EverandThe Ultimate Guide To Memory Improvement TechniquesPenilaian: 5 dari 5 bintang5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 5 dari 5 bintang5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDari EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisPenilaian: 5 dari 5 bintang5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 3.5 dari 5 bintang3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDari EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisPenilaian: 5 dari 5 bintang5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDari EverandThe Happiness Trap: How to Stop Struggling and Start LivingPenilaian: 4 dari 5 bintang4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDari EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifePenilaian: 4.5 dari 5 bintang4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDari EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsBelum ada peringkat
- The Tennis Partner: A Doctor's Story of Friendship and LossDari EverandThe Tennis Partner: A Doctor's Story of Friendship and LossPenilaian: 4.5 dari 5 bintang4.5/5 (4)