Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Controlling AngerDokumen36 halamanControlling Angerfau fauBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Helping Children Cope With DivorceDokumen6 halamanHelping Children Cope With Divorcedali77100% (2)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Melancholia A Disorder of Movement and Mood A Phenomenological and Neurobiological Review PDFDokumen353 halamanMelancholia A Disorder of Movement and Mood A Phenomenological and Neurobiological Review PDFPer SabBelum ada peringkat
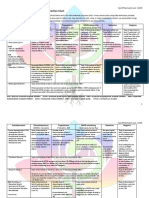
- Drug Interaction Chart for Antidepressants and PsychedelicsDokumen3 halamanDrug Interaction Chart for Antidepressants and PsychedelicsFred The Nomad100% (2)
- Psychiatry HistoryDokumen53 halamanPsychiatry HistoryMarco Góis100% (5)
- Why I Like The HospitalDokumen25 halamanWhy I Like The HospitalRahul Sharma100% (1)
- Communication Studies IA ExpositoryDokumen2 halamanCommunication Studies IA ExpositoryShania HaroldBelum ada peringkat
- Strange Stories TestDokumen359 halamanStrange Stories TestАлексейBelum ada peringkat
- Diagnosis Dan Penatalaksanaan Glaukoma1Dokumen12 halamanDiagnosis Dan Penatalaksanaan Glaukoma1Fahima AlbaarBelum ada peringkat
- Gangguan Tic TransienDokumen1 halamanGangguan Tic TransienMukhtar TarBelum ada peringkat
- Spinal DosingDokumen6 halamanSpinal DosingMukhtar TarBelum ada peringkat
- Malaria: Similarity Index Internet Sources Publications Student PapersDokumen3 halamanMalaria: Similarity Index Internet Sources Publications Student PapersMukhtar TarBelum ada peringkat
- Who AntroDokumen4 halamanWho AntroMukhtar TarBelum ada peringkat
- Social PhobiaDokumen10 halamanSocial PhobiaMukhtar TarBelum ada peringkat
- Gangguan Tic TransienDokumen1 halamanGangguan Tic TransienMukhtar TarBelum ada peringkat
- 2015 Article 516Dokumen12 halaman2015 Article 516Mukhtar TarBelum ada peringkat
- Burnout and Depression (Dentists)Dokumen9 halamanBurnout and Depression (Dentists)FranzBelum ada peringkat
- Name: MD Asif Bin Zahir Topic Tentative Title ID: 1731701630Dokumen7 halamanName: MD Asif Bin Zahir Topic Tentative Title ID: 1731701630Farhin AliBelum ada peringkat
- Validation of Forgiveness Scale and A Survey On The Relationship of Forgiveness and Students' Mental HealthDokumen8 halamanValidation of Forgiveness Scale and A Survey On The Relationship of Forgiveness and Students' Mental HealthFathima GaniBelum ada peringkat
- Name: Muhammad Jazim Reg # L1F20BSCE0024 Subject: English - II Depression in The TeenageDokumen2 halamanName: Muhammad Jazim Reg # L1F20BSCE0024 Subject: English - II Depression in The TeenageM jazimBelum ada peringkat
- Behavioral AnalysisDokumen125 halamanBehavioral AnalysisAnonymous XvwKtnSrMRBelum ada peringkat
- Mood-Disorders-SuicideDokumen67 halamanMood-Disorders-Suicidethe lousy donutBelum ada peringkat
- Psychological Well-Being and Smartphone Use Among College StudentsDokumen14 halamanPsychological Well-Being and Smartphone Use Among College StudentsIshika JainBelum ada peringkat
- Elizabeth Kawesa Dissertation Social Support Coping Depression and Subjective Wellbeing Among ASD Caregivers PDFDokumen88 halamanElizabeth Kawesa Dissertation Social Support Coping Depression and Subjective Wellbeing Among ASD Caregivers PDFwqewqewrewBelum ada peringkat
- Different Views of Anxiety DisordersDokumen380 halamanDifferent Views of Anxiety DisordersFrost Mai100% (2)
- Body Image in Children and Adolescents with CancerDokumen10 halamanBody Image in Children and Adolescents with CancerVanessa SilvaBelum ada peringkat
- Sexual Harassment On The InternetDokumen17 halamanSexual Harassment On The InternetdianerhanBelum ada peringkat
- Review of Related Literature and StudiesDokumen2 halamanReview of Related Literature and StudiesDerick MacedaBelum ada peringkat
- Moscovium Facts and Mental Health Strategies During PandemicDokumen13 halamanMoscovium Facts and Mental Health Strategies During PandemicRic Anthony LayasanBelum ada peringkat
- Psychiatric Disorders in Medical Practice: Specific SyndromesDokumen14 halamanPsychiatric Disorders in Medical Practice: Specific SyndromesEduard TomițaBelum ada peringkat
- The Problem and Its Background Introduction and Review of Related Literature and StudiesDokumen47 halamanThe Problem and Its Background Introduction and Review of Related Literature and StudiesCriza SorianoBelum ada peringkat
- Child Labor and Health: A Systematic Literature Review of The Impacts of Child Labor On Child 'S Health in Low-And Middle-Income CountriesDokumen9 halamanChild Labor and Health: A Systematic Literature Review of The Impacts of Child Labor On Child 'S Health in Low-And Middle-Income CountriesNabila IsnaniBelum ada peringkat
- Occupational Performance of Adolescents Drug Users PDFDokumen11 halamanOccupational Performance of Adolescents Drug Users PDFPaula FariaBelum ada peringkat
- Elder 20abuseDokumen27 halamanElder 20abusefebbuBelum ada peringkat
- Perfeccionismo e Insatisfacción Corpotal en Los Trastornos de Conducta AlimentariaDokumen12 halamanPerfeccionismo e Insatisfacción Corpotal en Los Trastornos de Conducta AlimentariaBrian Peña CaleroBelum ada peringkat
- Bibliotherapy: Helping Children Cope With Emotional and Developmental Distress Through Books Elizabeth Foss University of MarylandDokumen39 halamanBibliotherapy: Helping Children Cope With Emotional and Developmental Distress Through Books Elizabeth Foss University of MarylandRebecca MaryBelum ada peringkat
- Project 1 Expanded Middle New Research 1Dokumen4 halamanProject 1 Expanded Middle New Research 1api-595118101Belum ada peringkat
- Spini Et Al. (2017) A Life Course Framework For Studying VulnerabilityDokumen5 halamanSpini Et Al. (2017) A Life Course Framework For Studying VulnerabilityHayley WongBelum ada peringkat