Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Individualized Education PlanDokumen7 halamanIndividualized Education PlanElaine Aninang Hupeda100% (2)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Kuan Yin 100 Divine Lots InterpretationDokumen30 halamanKuan Yin 100 Divine Lots InterpretationEsperanza Theiss100% (2)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- S6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Dokumen26 halamanS6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Rona Dindang100% (1)
- 6.water Treatment and Make-Up Water SystemDokumen18 halaman6.water Treatment and Make-Up Water Systempepenapao1217100% (1)
- SCAT Chart - Systematic Cause Analysis Technique - SCAT ChartDokumen6 halamanSCAT Chart - Systematic Cause Analysis Technique - SCAT ChartSalman Alfarisi100% (1)
- bRAIN gYMDokumen11 halamanbRAIN gYMshannay201050% (2)
- Centor ScoreDokumen8 halamanCentor ScoreLoo DonBelum ada peringkat
- 10 1 1 563 4316 PDFDokumen5 halaman10 1 1 563 4316 PDFAuliaRahmanBelum ada peringkat
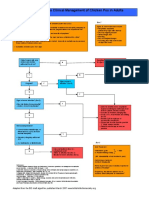
- Chicken Pox Guidelines PDFDokumen1 halamanChicken Pox Guidelines PDFAuliaRahmanBelum ada peringkat
- Post-Cardiac Arrest SyndromeDokumen30 halamanPost-Cardiac Arrest SyndromeAuliaRahmanBelum ada peringkat
- Centor ScoreDokumen8 halamanCentor ScoreLoo DonBelum ada peringkat
- RHDDokumen130 halamanRHDDeepu RajendranBelum ada peringkat
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDokumen22 halaman2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanBelum ada peringkat
- Anamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPDokumen4 halamanAnamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPAuliaRahmanBelum ada peringkat
- VACTERL-association EN PDFDokumen12 halamanVACTERL-association EN PDFAuliaRahmanBelum ada peringkat
- Anamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPDokumen4 halamanAnamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPAuliaRahmanBelum ada peringkat
- Who TRS 923 PDFDokumen130 halamanWho TRS 923 PDFAuliaRahmanBelum ada peringkat
- Jurnal OkeDokumen8 halamanJurnal OkeAuliaRahmanBelum ada peringkat
- Chicken Pox Guidelines PDFDokumen1 halamanChicken Pox Guidelines PDFAuliaRahmanBelum ada peringkat
- NEWSDokumen183 halamanNEWSSebastian BaqueroBelum ada peringkat
- Syarah Hikam 1Dokumen108 halamanSyarah Hikam 1AuliaRahmanBelum ada peringkat
- Interesting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaDokumen31 halamanInteresting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaAuliaRahmanBelum ada peringkat
- Varicella Vaccination AlgorithmDokumen1 halamanVaricella Vaccination AlgorithmAuliaRahmanBelum ada peringkat
- Igra Factsheet Oct2011 PDFDokumen2 halamanIgra Factsheet Oct2011 PDFAuliaRahmanBelum ada peringkat
- Incase Qobam Lab 17 MaretDokumen6 halamanIncase Qobam Lab 17 MaretAuliaRahmanBelum ada peringkat
- Interesting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaDokumen31 halamanInteresting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaAuliaRahmanBelum ada peringkat
- Wilayah 3'-DiterjemahkanDokumen1 halamanWilayah 3'-DiterjemahkanAuliaRahmanBelum ada peringkat
- Interesting Case 27.03.2013Dokumen10 halamanInteresting Case 27.03.2013AuliaRahmanBelum ada peringkat
- Makalah Brain GYM International, BDokumen17 halamanMakalah Brain GYM International, BAuliaRahmanBelum ada peringkat
- Breastfeeding: Best For Baby and MotherDokumen12 halamanBreastfeeding: Best For Baby and MotherSari Whardani Mahligai PateryBelum ada peringkat
- Diagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyDokumen24 halamanDiagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyAuliaRahmanBelum ada peringkat
- Diagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyDokumen24 halamanDiagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyAuliaRahmanBelum ada peringkat
- Pediatric Dental CareDokumen27 halamanPediatric Dental CareAuliaRahmanBelum ada peringkat
- Interesting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaDokumen10 halamanInteresting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaAuliaRahmanBelum ada peringkat
- Arecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionDokumen23 halamanArecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionNamae BacalBelum ada peringkat
- Mole Concept: Chemfile Mini-Guide To Problem SolvingDokumen18 halamanMole Concept: Chemfile Mini-Guide To Problem SolvingNaren ParasharBelum ada peringkat
- Lesson 8 - Philippine Disaster Risk Reduction and Management SystemDokumen11 halamanLesson 8 - Philippine Disaster Risk Reduction and Management SystemMary Joy CuetoBelum ada peringkat
- CV Dang Hoang Du - 2021Dokumen7 halamanCV Dang Hoang Du - 2021Tran Khanh VuBelum ada peringkat
- Deadline Anchors BrochureDokumen3 halamanDeadline Anchors Brochurejlmunozv100% (2)
- Regulation of Body FluidsDokumen7 halamanRegulation of Body FluidsRuth FamillaranBelum ada peringkat
- Limetas Maximos ResidualesDokumen27 halamanLimetas Maximos ResidualesXjoelx Olaya GonzalesBelum ada peringkat
- Human Resources Management Article Review On "The 3 Essential Jobs That Most Retention Programs Ignore"Dokumen14 halamanHuman Resources Management Article Review On "The 3 Essential Jobs That Most Retention Programs Ignore"Pang Kok ShengBelum ada peringkat
- Yanagiba Sharpening: Everything You Need To KnowDokumen16 halamanYanagiba Sharpening: Everything You Need To KnowT ChenBelum ada peringkat
- Ulcus Decubitus PDFDokumen9 halamanUlcus Decubitus PDFIrvan FathurohmanBelum ada peringkat
- Liquid - Liquid ExtractionDokumen19 halamanLiquid - Liquid ExtractionApurba Sarker ApuBelum ada peringkat
- Khatr Khola ISP District RatesDokumen56 halamanKhatr Khola ISP District RatesCivil EngineeringBelum ada peringkat
- The Congressional Committee and Philippine Policymaking: The Case of The Anti-Rape Law - Myrna LavidesDokumen29 halamanThe Congressional Committee and Philippine Policymaking: The Case of The Anti-Rape Law - Myrna LavidesmarielkuaBelum ada peringkat
- 3.SAFA AOCS 4th Ed Ce 2-66 1994Dokumen6 halaman3.SAFA AOCS 4th Ed Ce 2-66 1994Rofiyanti WibowoBelum ada peringkat
- NMC Confirmation FormDokumen3 halamanNMC Confirmation FormGianina AvasiloaieBelum ada peringkat
- Undas Deployment PadsDokumen15 halamanUndas Deployment PadsVic NairaBelum ada peringkat
- Informática Ejercicios IDokumen10 halamanInformática Ejercicios IAlejandroMendezBelum ada peringkat
- BOD FormatDokumen4 halamanBOD FormatSkill IndiaBelum ada peringkat
- 4Dokumen130 halaman4Upender BhatiBelum ada peringkat
- Baileys in 2009: Case Study Reference No 509-050-1Dokumen17 halamanBaileys in 2009: Case Study Reference No 509-050-1Ernesto KulasinBelum ada peringkat
- Lobby DirectoryDokumen3 halamanLobby DirectoryCathy AgamataBelum ada peringkat
- TSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideDokumen6 halamanTSB 20230831 - Reconnect FATL WM Error Code & Troubleshooting GuideNavjot KaurBelum ada peringkat
- DOC023.97.80076 - 3ed Sensores ORPDokumen148 halamanDOC023.97.80076 - 3ed Sensores ORPAlejandroBelum ada peringkat
- Climate Change and Global Warming and Its Impact On BangladeshDokumen7 halamanClimate Change and Global Warming and Its Impact On BangladeshAminulHoqueBelum ada peringkat
- Rainer M. Holm-Hadulla, Alina Bertolino: Use of Drugs by Jazz MusiciansDokumen3 halamanRainer M. Holm-Hadulla, Alina Bertolino: Use of Drugs by Jazz MusiciansTitikshaBelum ada peringkat