Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Gottfried, Marcuse FactorDokumen8 halamanGottfried, Marcuse Factoradorno65Belum ada peringkat
- The Veritas Handbook Final VersionDokumen347 halamanThe Veritas Handbook Final VersionThe Veritas Handbook100% (5)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Amigable vs. Cuenca DigestDokumen2 halamanAmigable vs. Cuenca Digestunbeatable38100% (5)
- Nelson Mandela's Leadership and Anti-Apartheid StruggleDokumen34 halamanNelson Mandela's Leadership and Anti-Apartheid StruggleAmmara Khalid100% (1)
- Letter Writing - Useful PhrasesDokumen3 halamanLetter Writing - Useful PhrasesLewis Enim100% (4)
- Padua Vs PeopleDokumen1 halamanPadua Vs PeopleKlaire EsdenBelum ada peringkat
- Baybay Water District v. COADokumen19 halamanBaybay Water District v. COAPlaneteer PranaBelum ada peringkat
- 2015 Materials On Criminal Law by Judge Campanilla UP Law CenterDokumen66 halaman2015 Materials On Criminal Law by Judge Campanilla UP Law CenterYan Rodriguez Dasal100% (12)
- OCA Vs GarongDokumen3 halamanOCA Vs GarongJeraldine Mae RaotraotBelum ada peringkat
- New Concepts in Orthodontics, Occlusion and TMJ DysfunctionDokumen8 halamanNew Concepts in Orthodontics, Occlusion and TMJ DysfunctionsorcBelum ada peringkat
- New Concepts in Orthodontics, Occlusion and TMJ DysfunctionDokumen8 halamanNew Concepts in Orthodontics, Occlusion and TMJ DysfunctionsorcBelum ada peringkat
- CH 21 Answer To in Class Diiscussion ProblemsDokumen20 halamanCH 21 Answer To in Class Diiscussion ProblemsJakeChavezBelum ada peringkat
- Dentsply GAC - CatalogDokumen336 halamanDentsply GAC - Catalogsorc50% (2)
- PDFDokumen7 halamanPDFsorcBelum ada peringkat
- BrosutaDokumen28 halamanBrosutasorcBelum ada peringkat
- Eng SubjectsDokumen25 halamanEng SubjectssorcBelum ada peringkat
- Symposium 2017 Pforzheim en NewDokumen28 halamanSymposium 2017 Pforzheim en NewsorcBelum ada peringkat
- TMJ 2015 PDFDokumen8 halamanTMJ 2015 PDFsorcBelum ada peringkat
- CCO Patient Diagnostic Sheet v6Dokumen2 halamanCCO Patient Diagnostic Sheet v6sorcBelum ada peringkat
- The Influence of Cranio-Cervical Posture On Maximal Mouth Opening and Pressure Pain Threshold in Patients With Myofascial Temporomandibular Pain DisordersDokumen8 halamanThe Influence of Cranio-Cervical Posture On Maximal Mouth Opening and Pressure Pain Threshold in Patients With Myofascial Temporomandibular Pain DisordersFelipeVidalBelum ada peringkat
- TMJ 2015Dokumen8 halamanTMJ 2015sorcBelum ada peringkat
- CCO Patient Diagnostic Sheet (Breakdown)Dokumen1 halamanCCO Patient Diagnostic Sheet (Breakdown)sorcBelum ada peringkat
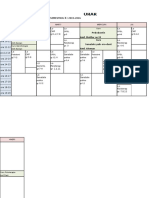
- Orar An 6 MD Seria 1 Sem LL 2015-2016Dokumen2 halamanOrar An 6 MD Seria 1 Sem LL 2015-2016sorcBelum ada peringkat
- AsdwDokumen56 halamanAsdwsorcBelum ada peringkat
- Spofa Catalogue en 2013 2014Dokumen59 halamanSpofa Catalogue en 2013 2014sorcBelum ada peringkat
- In OvationRArticlebyJerryClark IncreasingEfficiencyandProfitwithSelf LigatingBracketsDokumen5 halamanIn OvationRArticlebyJerryClark IncreasingEfficiencyandProfitwithSelf LigatingBracketssorcBelum ada peringkat
- 6a4 Cements en LowDokumen2 halaman6a4 Cements en LowsorcBelum ada peringkat
- JFLS-20 Item - 2013-05-12Dokumen1 halamanJFLS-20 Item - 2013-05-12sorcBelum ada peringkat
- Nihms 695420fgdfgDokumen40 halamanNihms 695420fgdfgsorcBelum ada peringkat
- Over The Last 2 Weeks, How Often Have You Been Bothered by The Following Problems? Place A Check Mark in The Box To Indicate Your AnswerDokumen1 halamanOver The Last 2 Weeks, How Often Have You Been Bothered by The Following Problems? Place A Check Mark in The Box To Indicate Your AnswersorcBelum ada peringkat
- Oral Behavior Checklist - 2013!05!12Dokumen1 halamanOral Behavior Checklist - 2013!05!12sorcBelum ada peringkat
- Graded Chronic Pain v2 - 1 Month - 2013!05!12Dokumen1 halamanGraded Chronic Pain v2 - 1 Month - 2013!05!12sorcBelum ada peringkat
- Nihms 695420fgdfgDokumen40 halamanNihms 695420fgdfgsorcBelum ada peringkat
- Patient Health Questionnaire-15: Physical SymptomsDokumen1 halamanPatient Health Questionnaire-15: Physical SymptomssorcBelum ada peringkat
- Oral Behavior Checklist - 2013!05!12Dokumen1 halamanOral Behavior Checklist - 2013!05!12sorcBelum ada peringkat
- Oral Behavior Checklist - 2013!05!12Dokumen1 halamanOral Behavior Checklist - 2013!05!12sorcBelum ada peringkat
- Graded Chronic Pain v2 - 1 Month - 2013!05!12mnbDokumen1 halamanGraded Chronic Pain v2 - 1 Month - 2013!05!12mnbsorcBelum ada peringkat
- DC-TMD Examform International 2013-05-12Dokumen2 halamanDC-TMD Examform International 2013-05-12sorcBelum ada peringkat
- JFLS-20 Item - 2013-05-12Dokumen1 halamanJFLS-20 Item - 2013-05-12sorcBelum ada peringkat
- How To Talk in An Arranged Marriage Meeting - 22 StepsDokumen3 halamanHow To Talk in An Arranged Marriage Meeting - 22 StepsqwertyasdfgBelum ada peringkat
- News You Can Use: 5-Star Resort 5-Star ResortDokumen56 halamanNews You Can Use: 5-Star Resort 5-Star ResortCoolerAds100% (5)
- Laws and Found: Phil Refining V, NG Sam DigestDokumen3 halamanLaws and Found: Phil Refining V, NG Sam DigestSilver Anthony Juarez PatocBelum ada peringkat
- ORDINANCE 2011-732: Code Providing For AnDokumen89 halamanORDINANCE 2011-732: Code Providing For AnThe Florida Times-UnionBelum ada peringkat
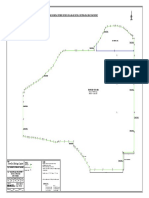
- Final Drawing in BUTM 2Dokumen1 halamanFinal Drawing in BUTM 2david46Belum ada peringkat
- Research Assignment 3 1Dokumen13 halamanResearch Assignment 3 1api-583942095Belum ada peringkat
- India S People S WarDokumen77 halamanIndia S People S WarSidhartha SamtaniBelum ada peringkat
- Cover Sheet: Month Day Month DayDokumen135 halamanCover Sheet: Month Day Month DayMichael MertaBelum ada peringkat
- TDS-466 Chembetaine CGFDokumen1 halamanTDS-466 Chembetaine CGFFabianoBelum ada peringkat
- Activity DesignDokumen12 halamanActivity DesignIra mae NavarroBelum ada peringkat
- Preliminary Offering Memorandum - Offering 2117Dokumen290 halamanPreliminary Offering Memorandum - Offering 2117ElDisenso.com100% (1)
- Test Drive AgreementDokumen5 halamanTest Drive AgreementRedcorp_MarketingBelum ada peringkat
- Arriola vs. SandiganbayanDokumen16 halamanArriola vs. SandiganbayanKKCDIALBelum ada peringkat
- Acosta v. PlanDokumen2 halamanAcosta v. PlanShayne SiguaBelum ada peringkat
- Universal Banking in IndiaDokumen6 halamanUniversal Banking in IndiaashwanidusadhBelum ada peringkat
- Audit of Insurance CompanyDokumen11 halamanAudit of Insurance CompanyTOLENTINO, Joferose AluyenBelum ada peringkat
- Avaya AuraDokumen94 halamanAvaya AuraVladimir DikosavljevicBelum ada peringkat
- Unit 3 Residential StatusDokumen41 halamanUnit 3 Residential Status24.7upskill Lakshmi V100% (3)
- Recognition and Moral Obligation (Makale, Honneth)Dokumen21 halamanRecognition and Moral Obligation (Makale, Honneth)Berk Özcangiller100% (1)
- Facebook Rankwave LawsuitDokumen11 halamanFacebook Rankwave LawsuitTechCrunchBelum ada peringkat