Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The Musical Form Articulates The Traditional Division of The Sonnet Into Four QuatrainsDokumen16 halamanThe Musical Form Articulates The Traditional Division of The Sonnet Into Four QuatrainsfranelonBelum ada peringkat
- The Creative Development of Johann Sebastian Bach, Volume II PDFDokumen450 halamanThe Creative Development of Johann Sebastian Bach, Volume II PDFfranelon100% (10)
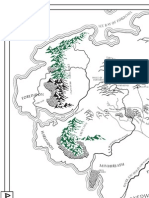
- MERP - Huge Middle Earth Map (6 Pages!) PDFDokumen6 halamanMERP - Huge Middle Earth Map (6 Pages!) PDFNightwings_brBelum ada peringkat
- A Heinrich Schütz Reader - Letters and Documents in Translation PDFDokumen324 halamanA Heinrich Schütz Reader - Letters and Documents in Translation PDFfranelon100% (1)
- Collections, Bars and Numbers: Analytical Coincidence or Bach's Design?Dokumen22 halamanCollections, Bars and Numbers: Analytical Coincidence or Bach's Design?franelonBelum ada peringkat
- A Conductor's Guide To Selected Baroque Choral-OrchestralDokumen272 halamanA Conductor's Guide To Selected Baroque Choral-Orchestralfranelon100% (1)
- Sibelius - Snöfrid VsDokumen20 halamanSibelius - Snöfrid VsfranelonBelum ada peringkat
- Heinichen, Rameau, and The Italian Thoroughbass Tradition - Concepts of Tonality and Chord inDokumen46 halamanHeinichen, Rameau, and The Italian Thoroughbass Tradition - Concepts of Tonality and Chord infranelonBelum ada peringkat
- Handel's Peace Anthem: Analysis of the MusicDokumen4 halamanHandel's Peace Anthem: Analysis of the MusicfranelonBelum ada peringkat
- C.P.E. Bachs Evangelist Johann HeinrichDokumen24 halamanC.P.E. Bachs Evangelist Johann HeinrichfranelonBelum ada peringkat
- (Doi 10.1093/earlyj/XXVIII.2.308) D. Burrows - Handel Oratorios (And L'Allegro)Dokumen3 halaman(Doi 10.1093/earlyj/XXVIII.2.308) D. Burrows - Handel Oratorios (And L'Allegro)franelonBelum ada peringkat
- TotentanzDokumen26 halamanTotentanzfranelonBelum ada peringkat
- Harpsichord in ContinuoDokumen11 halamanHarpsichord in ContinuofranelonBelum ada peringkat
- (Doi 10.1093/earlyj/XXVIII.2.308) D. Burrows - Handel Oratorios (And L'Allegro)Dokumen3 halaman(Doi 10.1093/earlyj/XXVIII.2.308) D. Burrows - Handel Oratorios (And L'Allegro)franelonBelum ada peringkat
- (Doi 10.1093/earlyj/XXVIII.2.308) D. Burrows - Handel Oratorios (And L'Allegro)Dokumen3 halaman(Doi 10.1093/earlyj/XXVIII.2.308) D. Burrows - Handel Oratorios (And L'Allegro)franelonBelum ada peringkat
- Acta Musicologica Volume 64 Issue 2 1992 (Doi 10.2307/932913) Jeanne Swack - Telemann Research Since 1975Dokumen27 halamanActa Musicologica Volume 64 Issue 2 1992 (Doi 10.2307/932913) Jeanne Swack - Telemann Research Since 1975franelonBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Chemistry Project Class XIIDokumen19 halamanChemistry Project Class XIISharvari ThakareBelum ada peringkat
- Fapcii DirectoryDokumen26 halamanFapcii DirectorysushantBelum ada peringkat
- The Human Superorganism - of Microbes and Men.Dokumen2 halamanThe Human Superorganism - of Microbes and Men.João SoaresBelum ada peringkat
- Rna Processing EukaryotesDokumen33 halamanRna Processing EukaryotesNathanaelBelum ada peringkat
- Immunology - Study Guide For Exam 1Dokumen1 halamanImmunology - Study Guide For Exam 1Danny Mills AnyikaBelum ada peringkat
- Split GeneDokumen27 halamanSplit Genemanojitchatterjee2007Belum ada peringkat
- DNA Extraction (Using The Omega Biotek E.Z.N.A. Mollusc DNA Kit)Dokumen3 halamanDNA Extraction (Using The Omega Biotek E.Z.N.A. Mollusc DNA Kit)xicoalexandreBelum ada peringkat
- Naghmana Bajwa, M.D. Recognized As A VIP Member by Strathmore's Who's Who Worldwide PublicationDokumen3 halamanNaghmana Bajwa, M.D. Recognized As A VIP Member by Strathmore's Who's Who Worldwide PublicationPR.comBelum ada peringkat
- Research Methodology Scheme and Syllabus For BBT and BBIDokumen3 halamanResearch Methodology Scheme and Syllabus For BBT and BBIShashi KumarBelum ada peringkat
- Coursera BioinfoMethods-II Lab02Dokumen14 halamanCoursera BioinfoMethods-II Lab02Alex ChenBelum ada peringkat
- Endothelin-1 Gene Regulation: The FASEB JournalDokumen13 halamanEndothelin-1 Gene Regulation: The FASEB JournalElena EllaBelum ada peringkat
- Company Details in APDokumen8 halamanCompany Details in APJeyaraman BaskaranBelum ada peringkat
- Curriculum Vitae FinalDokumen5 halamanCurriculum Vitae FinalNandini JoshiBelum ada peringkat
- Fungi As Biocontrol Agents - 20130410 - 173915Dokumen401 halamanFungi As Biocontrol Agents - 20130410 - 173915Nelver MorenoBelum ada peringkat
- Universal Haplotype-Based Noninvasive Prenatal Testing For Single Gene DiseasesDokumen12 halamanUniversal Haplotype-Based Noninvasive Prenatal Testing For Single Gene DiseasestestBelum ada peringkat
- Lab FacilitiesDokumen2 halamanLab FacilitiesSelvakapoorBelum ada peringkat
- Molecular Biology of The Cell - NCBI BookshelfDokumen7 halamanMolecular Biology of The Cell - NCBI Bookshelfstaryk100% (1)
- Hot Biotech Startups LowresDokumen27 halamanHot Biotech Startups LowreschetanudctBelum ada peringkat
- Bayer Organizational Structure 2011 02 01Dokumen1 halamanBayer Organizational Structure 2011 02 01jessica0% (1)
- Cultural Characterization of MicroorganismsDokumen3 halamanCultural Characterization of MicroorganismsABelum ada peringkat
- Isolation of Bacterial Plasmid DNA (Compatibility Mode)Dokumen18 halamanIsolation of Bacterial Plasmid DNA (Compatibility Mode)Khandoker Faisal100% (1)
- Supercos 1 Cosmid Vector Kit: Instruction ManualDokumen27 halamanSupercos 1 Cosmid Vector Kit: Instruction Manualkatia sarmiento bujatoBelum ada peringkat
- KOD - Plus-Neo: Store at - 20°CDokumen12 halamanKOD - Plus-Neo: Store at - 20°CArga GuruBelum ada peringkat
- 12-O-Tetradecanoylphorbol-13 - Acetate (TPA) Is Anti-Tumorigenic in Liver Cancer Cells Via Inhibiting YAP Through AMOT-srep44940Dokumen11 halaman12-O-Tetradecanoylphorbol-13 - Acetate (TPA) Is Anti-Tumorigenic in Liver Cancer Cells Via Inhibiting YAP Through AMOT-srep44940harrybzyBelum ada peringkat
- Biology Chapter 21 Sylvia Mader ModifiedDokumen29 halamanBiology Chapter 21 Sylvia Mader ModifiedabdallahBelum ada peringkat
- Assessment and Determination of Optimum Concentration of Streptomycin and Kanamycin As Selective Agents in Peppermint (MenthaDokumen6 halamanAssessment and Determination of Optimum Concentration of Streptomycin and Kanamycin As Selective Agents in Peppermint (MenthaMonaia YehiaBelum ada peringkat
- Formulas QuimicasDokumen331 halamanFormulas QuimicasNelver MorenoBelum ada peringkat
- PenicillinDokumen75 halamanPenicillinJean CabigaoBelum ada peringkat
- Maa Rampyari Super Speciality Hospital Doc. No. E / Nabh / MRPSH / Fms / 1Dokumen4 halamanMaa Rampyari Super Speciality Hospital Doc. No. E / Nabh / MRPSH / Fms / 1tanishaBelum ada peringkat
- Globin Synthesis PDFDokumen6 halamanGlobin Synthesis PDFmanoj_rkl_07100% (1)