Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Handwriting Protocol August 2009 FinalDokumen62 halamanHandwriting Protocol August 2009 FinalTeresa Caba Gallego100% (6)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Occupational Therapy Discontinuation ReportDokumen2 halamanOccupational Therapy Discontinuation Reportapi-273311864Belum ada peringkat
- The Intentional Relationship ModelDokumen6 halamanThe Intentional Relationship ModelmkecikBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- 7 Behavioral Cognitive ContinuumDokumen20 halaman7 Behavioral Cognitive Continuumsaleemahamed88100% (1)
- Ot Final Project 3Dokumen3 halamanOt Final Project 3api-339841373Belum ada peringkat
- Occupational Therapy ProcessDokumen3 halamanOccupational Therapy Processapi-339841373100% (1)
- DomainandprocessDokumen3 halamanDomainandprocessapi-339841373Belum ada peringkat
- Intro To Ot FinalDokumen3 halamanIntro To Ot Finalapi-339841373Belum ada peringkat
- 13 OT Occup Rehab AOTA Exam PrepDokumen17 halaman13 OT Occup Rehab AOTA Exam PrepThirdy BullerBelum ada peringkat
- Depression Children PDFDokumen2 halamanDepression Children PDFConstanzaBelum ada peringkat
- Test Bank For Basic Nursing by TreasDokumen36 halamanTest Bank For Basic Nursing by Treasfraughtoutlay1dknw0100% (41)
- BY P.Preethika BSC-15-26 3 BSC Psychology Psychopathology AssignmentDokumen15 halamanBY P.Preethika BSC-15-26 3 BSC Psychology Psychopathology AssignmentpreethikaBelum ada peringkat
- Ot Promotion AssignmentDokumen6 halamanOt Promotion Assignmentapi-538972374Belum ada peringkat
- A Grounded Theory Analysis of The Relationship Between Creativity and Occupational TherapyDokumen389 halamanA Grounded Theory Analysis of The Relationship Between Creativity and Occupational TherapyAngela EnacheBelum ada peringkat
- 7117468608Dokumen3 halaman7117468608علاء يحييBelum ada peringkat
- Splinting For The Prevention Correction of Contractures in Adults With Neurological Dysfunction Quick ReferDokumen12 halamanSplinting For The Prevention Correction of Contractures in Adults With Neurological Dysfunction Quick ReferDaniel MarvasoBelum ada peringkat
- OT and Eating DysfunctionDokumen1 halamanOT and Eating DysfunctionMCris EsSemBelum ada peringkat
- My Library StudyDokumen47 halamanMy Library Studyangel vermaBelum ada peringkat
- FinalstatementofintentDokumen1 halamanFinalstatementofintentapi-546274167Belum ada peringkat
- Information Brochure - CET 2023Dokumen27 halamanInformation Brochure - CET 2023African HadidiBelum ada peringkat
- Chapter 19 Chemotherapy-Induced Peripheral NeuropathyDokumen13 halamanChapter 19 Chemotherapy-Induced Peripheral Neuropathyapi-519320173Belum ada peringkat
- Occupational Therapy in Disaster Preparedness and Response DPRDokumen2 halamanOccupational Therapy in Disaster Preparedness and Response DPRerlitaBelum ada peringkat
- Autism Paper Final DraftDokumen13 halamanAutism Paper Final Draftapi-467824609Belum ada peringkat
- Times Review Classifieds: March 24, 2016Dokumen8 halamanTimes Review Classifieds: March 24, 2016TimesreviewBelum ada peringkat
- Multicultural in Counseling - 1Dokumen11 halamanMulticultural in Counseling - 1sarahariffin001Belum ada peringkat
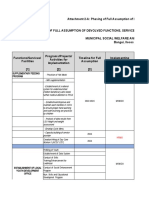
- MSWDO Capdev Form G1 FINALDokumen50 halamanMSWDO Capdev Form G1 FINALbai yhang de la cruz100% (1)
- Early Intervention FAQDokumen7 halamanEarly Intervention FAQSara Gomes CastroBelum ada peringkat
- Sarah Jean Barton CV July 2020Dokumen11 halamanSarah Jean Barton CV July 2020Andrew PhillipsBelum ada peringkat
- Pool Activity Level (PAL) Instrument For Occupational ProfilingDokumen35 halamanPool Activity Level (PAL) Instrument For Occupational ProfilingAngela GohBelum ada peringkat
- Demi Moses ResumeDokumen1 halamanDemi Moses Resumeapi-403058257Belum ada peringkat
- Rachel Bray - ResumeDokumen2 halamanRachel Bray - Resumeapi-625221885Belum ada peringkat
- Psychiatric and Mental Health NursingDokumen19 halamanPsychiatric and Mental Health NursingAbeer salehBelum ada peringkat
- Boardroom To ClassroomDokumen1 halamanBoardroom To ClassroomThe American Occupational Therapy AssociationBelum ada peringkat
- Ot Process NotesDokumen2 halamanOt Process NotesFrancesBelum ada peringkat