Anda mungkin juga menyukai
- Coronary Vasomotion AbnormalitiesDari EverandCoronary Vasomotion AbnormalitiesHiroaki ShimokawaBelum ada peringkat
- Posterior Circulation Stroke: Advances in Understanding and ManagementDari EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimBelum ada peringkat
- Specific Heart Muscle DiseaseDari EverandSpecific Heart Muscle DiseaseCecil SymonsBelum ada peringkat
- Cardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesDari EverandCardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesBelum ada peringkat
- Clinical Cases in Heart FailureDari EverandClinical Cases in Heart FailureRavi V. ShahBelum ada peringkat
- Cellular and Molecular Pathobiology of Cardiovascular DiseaseDari EverandCellular and Molecular Pathobiology of Cardiovascular DiseaseMonte WillisBelum ada peringkat
- Cardiorenal Syndrome in Heart FailureDari EverandCardiorenal Syndrome in Heart FailureW. H. Wilson TangBelum ada peringkat
- MINOCA Agewall 2017Dokumen11 halamanMINOCA Agewall 2017mate ellaBelum ada peringkat
- Arrhythmic SyncopeDokumen24 halamanArrhythmic Syncopebagus joyoBelum ada peringkat
- Translational Research in Coronary Artery Disease: Pathophysiology to TreatmentDari EverandTranslational Research in Coronary Artery Disease: Pathophysiology to TreatmentBelum ada peringkat
- Characteristics of Coronary Artery Disease Among Patients With Atrial Fibrillation Compared To Patients With Sinus RhythmDokumen9 halamanCharacteristics of Coronary Artery Disease Among Patients With Atrial Fibrillation Compared To Patients With Sinus RhythmFaisal AdamBelum ada peringkat
- Coronary Artery Disease Literature ReviewDokumen4 halamanCoronary Artery Disease Literature Reviewaflsvwoeu100% (1)
- Microcirculation in Cardiovascular DiseasesDari EverandMicrocirculation in Cardiovascular DiseasesEnrico Agabiti-RoseiBelum ada peringkat
- Vascular Compression Syndromes - What You Need to KnowDari EverandVascular Compression Syndromes - What You Need to KnowBelum ada peringkat
- Yatsynovich 2017 Cardiac SarcoidosiDokumen64 halamanYatsynovich 2017 Cardiac SarcoidosiJohan ArocaBelum ada peringkat
- Early Vascular Aging (EVA): New Directions in Cardiovascular ProtectionDari EverandEarly Vascular Aging (EVA): New Directions in Cardiovascular ProtectionPedro Guimarães CunhaBelum ada peringkat
- Microcirculation: From Bench to BedsideDari EverandMicrocirculation: From Bench to BedsideMaria DorobantuBelum ada peringkat
- Acute Stroke Management in the Era of ThrombectomyDari EverandAcute Stroke Management in the Era of ThrombectomyEdgar A. SamaniegoBelum ada peringkat
- Nejmo. TAKOSUBO PDFDokumen10 halamanNejmo. TAKOSUBO PDFAny CórdovaBelum ada peringkat
- Chest Pain With Normal Coronary Arteries (2013)Dokumen350 halamanChest Pain With Normal Coronary Arteries (2013)Farly KerapBelum ada peringkat
- Ischemic Heart Disease Literature ReviewDokumen4 halamanIschemic Heart Disease Literature Reviewafdtvovhb100% (1)
- 2000 Bookmatter TextbookOfAngiologyDokumen19 halaman2000 Bookmatter TextbookOfAngiologydavidmarkovic032Belum ada peringkat
- Spondilita Ankilozanta Cardio PulmonarDokumen6 halamanSpondilita Ankilozanta Cardio PulmonarGiulia LungulescuBelum ada peringkat
- Intra Cath ArrythemiasDokumen17 halamanIntra Cath Arrythemiasmuath taaniBelum ada peringkat
- Penatalaksanaan Pemeriksaan Coronary Angiongraphy Pada KasusDokumen9 halamanPenatalaksanaan Pemeriksaan Coronary Angiongraphy Pada KasusJamy KarmanBelum ada peringkat
- Coronary Artery Disease An Example Case StudyDokumen19 halamanCoronary Artery Disease An Example Case StudyrumasadraunaBelum ada peringkat
- Spon Artery DissceDokumen6 halamanSpon Artery DissceMuhammad JunaidBelum ada peringkat
- Postural Tachycardia Syndrome: A Concise and Practical Guide to Management and Associated ConditionsDari EverandPostural Tachycardia Syndrome: A Concise and Practical Guide to Management and Associated ConditionsNicholas GallBelum ada peringkat
- Amyloidosis and ASDokumen15 halamanAmyloidosis and ASomarfaridtawfikBelum ada peringkat
- Practical Carotid Artery StentingDari EverandPractical Carotid Artery StentingSumaira MacdonaldBelum ada peringkat
- Diabetes and Peripheral Vascular Disease: Diagnosis and ManagementDari EverandDiabetes and Peripheral Vascular Disease: Diagnosis and ManagementBelum ada peringkat
- Management of Cardiac ArrhythmiasDari EverandManagement of Cardiac ArrhythmiasGan-Xin YanBelum ada peringkat
- AnginaDokumen18 halamanAnginabertouwBelum ada peringkat
- Clinical Handbook of Cardiac ElectrophysiologyDari EverandClinical Handbook of Cardiac ElectrophysiologyBenedict M. GloverBelum ada peringkat
- Essential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsDari EverandEssential Facts in Cardiovascular Medicine: Board Review and Clinical PearlsBelum ada peringkat
- Heart Failure Thesis PDFDokumen6 halamanHeart Failure Thesis PDFafknwride100% (2)
- Spontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionDokumen3 halamanSpontaneous Coronary Artery Dissection With Clinical Presentation of Acute Myocardial InfarctionSabrina JonesBelum ada peringkat
- Pepas de SC Post InfartoDokumen24 halamanPepas de SC Post InfartoJosé AñorgaBelum ada peringkat
- An Observational Study On Diastolic Function in Post Myocardial Infarction Patients in A Tertiary Care Centre in Kancheepuram DistrictDokumen7 halamanAn Observational Study On Diastolic Function in Post Myocardial Infarction Patients in A Tertiary Care Centre in Kancheepuram DistrictIJAR JOURNALBelum ada peringkat
- Ischemic 39!Dokumen6 halamanIschemic 39!Adina Alexandra CBelum ada peringkat
- Stable Angina MV SBDokumen11 halamanStable Angina MV SBAndi NamirahBelum ada peringkat
- Atherosclerosis: Clinical Perspectives Through ImagingDari EverandAtherosclerosis: Clinical Perspectives Through ImagingBelum ada peringkat
- Vasospastic Angina: A Literature Review of Current Evidence: SciencedirectDokumen12 halamanVasospastic Angina: A Literature Review of Current Evidence: SciencedirectMade ChandraBelum ada peringkat
- Screening and Management of Atrial Fibrillation in Primary Care InglesDokumen18 halamanScreening and Management of Atrial Fibrillation in Primary Care InglesIvan VelasquezBelum ada peringkat
- Fa BJM 2021Dokumen18 halamanFa BJM 2021Grisel MezaBelum ada peringkat
- Coronary Calcium: A Comprehensive Understanding of Its Biology, Use in Screening, and Interventional ManagementDari EverandCoronary Calcium: A Comprehensive Understanding of Its Biology, Use in Screening, and Interventional ManagementAloke Virmani FinnBelum ada peringkat
- A System Based' Approach To Risk Assessment of The Cervical Spine Prior ToDokumen9 halamanA System Based' Approach To Risk Assessment of The Cervical Spine Prior ToRudolfGerBelum ada peringkat
- Minoca - Are We Doing It Wrong?Dokumen6 halamanMinoca - Are We Doing It Wrong?khusnulBelum ada peringkat
- Klingel Caforio Eur Heart J2013Dokumen18 halamanKlingel Caforio Eur Heart J2013SarahBelum ada peringkat
- Thesis Acute Coronary SyndromeDokumen8 halamanThesis Acute Coronary Syndromeaflpcdwfunzfed100% (2)
- Prostaglandins, Platelets, Lipids: New Developments in AtherosclerosisDari EverandProstaglandins, Platelets, Lipids: New Developments in AtherosclerosisBelum ada peringkat
- Self-Assessment: BOFs for MRCP(UK) and MRCP(I) Part IDari EverandSelf-Assessment: BOFs for MRCP(UK) and MRCP(I) Part IBelum ada peringkat
- Acute Myocardial Infarction:: Pathophysiology and PresentationDokumen40 halamanAcute Myocardial Infarction:: Pathophysiology and PresentationSelecta Dejosep GonzalesBelum ada peringkat
- DR Vijay Amaranath, DM NIMS, HyderabadDokumen100 halamanDR Vijay Amaranath, DM NIMS, HyderabadJhonny CastilloBelum ada peringkat
- Goactive Policy DocumentDokumen50 halamanGoactive Policy Documentwaran RMBelum ada peringkat
- Cardiac RehabilitationDokumen5 halamanCardiac RehabilitationGian Carlo Poggi EscobarBelum ada peringkat
- Cardiac Rhythms - ECG ReadingsDokumen15 halamanCardiac Rhythms - ECG Readingsal-obinay shereenBelum ada peringkat
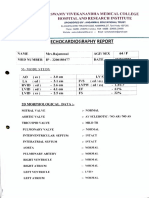
- ECOCARDIODokumen3 halamanECOCARDIOArun ComedsBelum ada peringkat
- Normal Sinus RhythmDokumen13 halamanNormal Sinus RhythmJackson Yovin ChellyadhasBelum ada peringkat
- 2014 AHA ACC Guideline For The Management VHDDokumen129 halaman2014 AHA ACC Guideline For The Management VHDshaeeBelum ada peringkat
- 5 Cardiac Cycle & Heart SoundsDokumen32 halaman5 Cardiac Cycle & Heart SoundsDisha SuvarnaBelum ada peringkat
- Hospital DetailsDokumen34 halamanHospital Detailsmolus030Belum ada peringkat
- Brunilda Alushi@Dokumen3 halamanBrunilda Alushi@brunilda.alushiBelum ada peringkat
- CardiologyDokumen345 halamanCardiologyClaudiu Ungureanu Clau100% (3)
- Lucknow Hospital OPD Schedule1Dokumen2 halamanLucknow Hospital OPD Schedule1Romesh KumarBelum ada peringkat
- Cardio My OpathiesDokumen61 halamanCardio My OpathiesIrina Cabac-PogoreviciBelum ada peringkat
- Reading 1Dokumen5 halamanReading 1Buiducanh BuiBelum ada peringkat
- 1 Part I CPR Q&ADokumen54 halaman1 Part I CPR Q&AYousaf LallarBelum ada peringkat
- Sono 338 - Echocardiography-Worksheet 2017Dokumen2 halamanSono 338 - Echocardiography-Worksheet 2017api-347648847Belum ada peringkat
- Tabel Obat Kardiovaskuler Aulia Nurtafani Reforma (189296)Dokumen9 halamanTabel Obat Kardiovaskuler Aulia Nurtafani Reforma (189296)Aulia Nurtafani ReformaBelum ada peringkat
- Right Ventricular Size and Function TucayDokumen50 halamanRight Ventricular Size and Function TucayDenisyamsuddinBelum ada peringkat
- Chapter 26 Dysrhythmias Quizlet 4Dokumen31 halamanChapter 26 Dysrhythmias Quizlet 4Marshin Thea CelociaBelum ada peringkat
- Physiology of The HeartDokumen27 halamanPhysiology of The HeartNavadeep KalluriBelum ada peringkat
- Cardiovascular ExaminationDokumen4 halamanCardiovascular ExaminationarchanaBelum ada peringkat
- Answers MediDokumen443 halamanAnswers MediAmine Younis100% (13)
- Cardiac Catheterization: Dr. Ravi Gadani MS, FmasDokumen50 halamanCardiac Catheterization: Dr. Ravi Gadani MS, FmasRaviBelum ada peringkat
- Soal MAYO Yg KeluarDokumen8 halamanSoal MAYO Yg KeluardoktersaktiBelum ada peringkat
- Comen DefibrilatorEN S5 V1.0Dokumen4 halamanComen DefibrilatorEN S5 V1.0alabasbsmBelum ada peringkat
- Journal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantDokumen12 halamanJournal of Arrhythmia - 2023 - Nagashima - Systematic Observation Based Diagnosis of Atrioventricular Nodal ReentrantSebastian ChandraBelum ada peringkat
- Care of Clients With Cardiovascular DisordersDokumen67 halamanCare of Clients With Cardiovascular DisordersMatt Lao DionelaBelum ada peringkat
- Graphic Organizer-Heart Murmur Elvis Baquero 7mo CDokumen3 halamanGraphic Organizer-Heart Murmur Elvis Baquero 7mo CEduardo AcostaBelum ada peringkat
- Cardiac Monitoring PDFDokumen7 halamanCardiac Monitoring PDFDelia LopBelum ada peringkat