Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- CIRS Guidelines On Perc Ablation Small Renal Cell CarcinomaDokumen15 halamanCIRS Guidelines On Perc Ablation Small Renal Cell CarcinomaRuminRuBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- TACE Standards of PracticeDokumen17 halamanTACE Standards of PracticeRuminRuBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Role of US in Acute PelvicDokumen17 halamanRole of US in Acute PelvicRuminRuBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Radiology Trauma Fracture BylDokumen6 halamanRadiology Trauma Fracture BylRuminRuBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Pancreas: Cynthia D. Guy, MD Associate Professor of Pathology DumcDokumen56 halamanPancreas: Cynthia D. Guy, MD Associate Professor of Pathology Dumcionut1ilie-1Belum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- CHAPTER 7 Review QuestionsDokumen5 halamanCHAPTER 7 Review QuestionsMia MistypuffBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
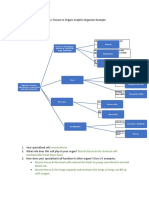
- Cells To Tissues To Organs Graphic Organizer ExampleDokumen2 halamanCells To Tissues To Organs Graphic Organizer Exampleapi-431603797Belum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- (Methods in Molecular Biology 1956) Ralf Küppers - Lymphoma - Methods and Protocols-Springer New York - Humana Press (2019)Dokumen439 halaman(Methods in Molecular Biology 1956) Ralf Küppers - Lymphoma - Methods and Protocols-Springer New York - Humana Press (2019)Enrique Guerrero100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Blood Group IncompatibilityDokumen7 halamanBlood Group IncompatibilityHendrikus Surya Adhi PutraBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Sistem Imun 2Dokumen20 halamanSistem Imun 2CameliaMasrijalBelum ada peringkat
- Skeletal System Janelyn 1Dokumen20 halamanSkeletal System Janelyn 1Lalaine BulutBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Anemia DX TXDokumen2 halamanAnemia DX TXProsanjit MajumderBelum ada peringkat
- Chapter 4Dokumen17 halamanChapter 4JohnBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- AVP Palatine Ulcers Article PDFDokumen5 halamanAVP Palatine Ulcers Article PDFartzain1991Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Plant CellDokumen22 halamanThe Plant CellLuna Scorpius0% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Lanat - Bsfi-3a - Module 2-AssessmentDokumen2 halamanLanat - Bsfi-3a - Module 2-AssessmentLemark Galban LanatBelum ada peringkat
- Obstetric Ultrasound Report FormatDokumen3 halamanObstetric Ultrasound Report Formatሀይደር ዶ.ር60% (5)
- Carrier-Mediated Dermal DeliveryDokumen587 halamanCarrier-Mediated Dermal DeliveryVanderval SIlva de OliveiraBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Connective Tissue GraftDokumen13 halamanConnective Tissue Graftdrkalpana jainBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- 2021-Review-Gut Microbiota in Cancer Immune Response and ImmunotherapyDokumen14 halaman2021-Review-Gut Microbiota in Cancer Immune Response and ImmunotherapyCristian Felipe Sandoval QuiñonezBelum ada peringkat
- 14 Sop Got Electric ShockDokumen3 halaman14 Sop Got Electric ShockRio SimatupangBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Form 2 Science Chapter 2 NutritionDokumen21 halamanForm 2 Science Chapter 2 NutritionCK100% (3)
- Melanoma MalignaDokumen28 halamanMelanoma MalignaDila Muflikhy PutriBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFDokumen18 halamanThe Theater of Anatomy - The Anatomical Preparations of Honore Fragonard PDFFrancisco SantosBelum ada peringkat
- Appendix DuplicationDokumen3 halamanAppendix DuplicationMario TrejoBelum ada peringkat
- Assessing The Skull and Face Eye Structures and Visual Acuity Ears and Hearing Nose and Sinuses Mouth and Oropharynx and Neck Basic ConceptDokumen23 halamanAssessing The Skull and Face Eye Structures and Visual Acuity Ears and Hearing Nose and Sinuses Mouth and Oropharynx and Neck Basic ConceptFrancar Jade De VeraBelum ada peringkat
- Cysts of The JawsDokumen75 halamanCysts of The JawsSwetha KaripineniBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Lecture 6 LungsDokumen14 halamanLecture 6 LungsOsama MalikBelum ada peringkat
- Functional Matrix HypothesisDokumen14 halamanFunctional Matrix Hypothesispriyab710Belum ada peringkat
- ANA205 Introduction To Embryology (Lecture 1) Enaibe 2019Dokumen35 halamanANA205 Introduction To Embryology (Lecture 1) Enaibe 2019DOUGLAS KIPRUTOBelum ada peringkat
- ICSE QUESTION PAPER Biology 2006 Class 10 PDFDokumen8 halamanICSE QUESTION PAPER Biology 2006 Class 10 PDFLokesh MalikBelum ada peringkat
- 8 Cell - The Unit of Life-Notes - SampleDokumen2 halaman8 Cell - The Unit of Life-Notes - SampleManish KumarBelum ada peringkat
- Respiratory SystemDokumen23 halamanRespiratory Systemjimboy baddiriBelum ada peringkat
- FNA Soft TX TuDokumen74 halamanFNA Soft TX TufadoBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)