Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The P.J. Nolan Snooker Coaching Guide (Senior) PDFDokumen30 halamanThe P.J. Nolan Snooker Coaching Guide (Senior) PDFAnonymous w4lLoMd7100% (4)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Aagaard & Ntirlis - PlayingtheFrench-excerptDokumen9 halamanAagaard & Ntirlis - PlayingtheFrench-excerptGustavo WalterBelum ada peringkat
- The Way of Seiryoku Zenyo-Jita Kyoei in JudoDokumen6 halamanThe Way of Seiryoku Zenyo-Jita Kyoei in JudoJohn Doe100% (1)
- Agile Outcome Measures Ems v2 PDFDokumen8 halamanAgile Outcome Measures Ems v2 PDFjusudBelum ada peringkat
- LBP MyogenikDokumen12 halamanLBP MyogenikDewiSukma'sBelum ada peringkat
- Subacromial Decompression Distal Clavicle ExcisionDokumen2 halamanSubacromial Decompression Distal Clavicle ExcisionDewiSukma'sBelum ada peringkat
- Ac ReconDokumen2 halamanAc ReconDewiSukma'sBelum ada peringkat
- 100m DashDokumen13 halaman100m Dashapi-283083678Belum ada peringkat
- Taboo Words - E-Sh Speak CountriesDokumen3 halamanTaboo Words - E-Sh Speak CountriesStellaGramaBelum ada peringkat
- Fundamental Dance StepsDokumen18 halamanFundamental Dance StepsJoseph Eric Nardo100% (1)
- How To Play Batu SerembanDokumen2 halamanHow To Play Batu SerembanKhadijahOmarBelum ada peringkat
- Pareto Chart: Basic Tools For Process ImprovementDokumen49 halamanPareto Chart: Basic Tools For Process ImprovementGirish RajBelum ada peringkat
- 1 - Tampa Bay Downs PPDokumen23 halaman1 - Tampa Bay Downs PPGregorioBelum ada peringkat
- 2019 Southeast Asian Games Cauldron PDFDokumen2 halaman2019 Southeast Asian Games Cauldron PDFPatricia Camille Nepomuceno MateoBelum ada peringkat
- NCAA07 Defensive Playbook FinalDokumen10 halamanNCAA07 Defensive Playbook Finaltjdendy100% (1)
- Phase+3+ +Bodyweight+ONLYDokumen11 halamanPhase+3+ +Bodyweight+ONLYCatalinBelum ada peringkat
- Spi Matches LatestDokumen675 halamanSpi Matches LatestClaudioGuttyBelum ada peringkat
- Mrinmay Kushal: Gnlu Cricket Quiz CircleDokumen24 halamanMrinmay Kushal: Gnlu Cricket Quiz CircleMRINMAY KUSHALBelum ada peringkat
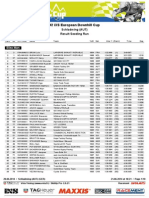
- Result Seeding Run Schladming2014Dokumen10 halamanResult Seeding Run Schladming2014racementBelum ada peringkat
- Abecedario y Tablas Llavero Tik TokDokumen6 halamanAbecedario y Tablas Llavero Tik TokAna SuarezBelum ada peringkat
- CR7 Vs MessiDokumen6 halamanCR7 Vs MessiNicolas Villa AlarconBelum ada peringkat
- Speaking Task For IELTSDokumen9 halamanSpeaking Task For IELTSMari FeroyanBelum ada peringkat
- Palawanseaexplorer CV-PortfolioDokumen3 halamanPalawanseaexplorer CV-PortfolioBen RiverBelum ada peringkat
- Aura Brochure PDFDokumen20 halamanAura Brochure PDFKunal Singh ShekhawatBelum ada peringkat
- Horses and Sport: Horse Sport Within Current European PolicymakingDokumen2 halamanHorses and Sport: Horse Sport Within Current European PolicymakingOrientación Juan ReyBelum ada peringkat
- Australian Guineas Day: Saturday 1 March 2014Dokumen2 halamanAustralian Guineas Day: Saturday 1 March 2014Flemington RacecourseBelum ada peringkat
- Dunbar Summer Series / Canada Cup DH #1 - Fernie, B.C.Dokumen10 halamanDunbar Summer Series / Canada Cup DH #1 - Fernie, B.C.Matthew PioroBelum ada peringkat
- Baseball SoftballDokumen156 halamanBaseball SoftballMaximilien LocqBelum ada peringkat
- World Chess Championships 1993Dokumen132 halamanWorld Chess Championships 1993José Rafael Córdova Rangel100% (11)
- Reaction Paper - Intramurals2022Dokumen1 halamanReaction Paper - Intramurals2022Krichelle Anne Escarilla II100% (1)
- 09-01-13 Andrea Tallarita - Understanding Italian Football (Part I) FantasiaDokumen4 halaman09-01-13 Andrea Tallarita - Understanding Italian Football (Part I) FantasiaskanzeniBelum ada peringkat
- E Bike Owners ManualDokumen16 halamanE Bike Owners ManualShrawan Kumar Jha100% (1)
- Grip Strength and ElectromyogramDokumen8 halamanGrip Strength and ElectromyogramChandra Murali100% (1)
- ESL/Brownies/Scouts Games & ActivitiesDokumen17 halamanESL/Brownies/Scouts Games & ActivitiesNiamh Ní ChinnéideBelum ada peringkat