Anda mungkin juga menyukai
- Anaphysio (Case Pres)Dokumen7 halamanAnaphysio (Case Pres)Ralph_John_Pac_8337Belum ada peringkat
- Maternal NursingDokumen130 halamanMaternal NursingChristine MatasBelum ada peringkat
- The Phases of Menstrual CycleDokumen5 halamanThe Phases of Menstrual CycleKristine AlejandroBelum ada peringkat
- External Female GenitalsDokumen4 halamanExternal Female GenitalsKim SunooBelum ada peringkat
- Maternal and Child Health Nursing Reviewer-CompleteDokumen66 halamanMaternal and Child Health Nursing Reviewer-Completeposh003892% (39)
- Anatomy and Physiology Reproductive System: ComponentsDokumen7 halamanAnatomy and Physiology Reproductive System: ComponentsMark Nel Nuñez100% (1)
- Anatomy and PhysiologyDokumen5 halamanAnatomy and PhysiologytwicetrashBelum ada peringkat
- Uterine Cycle...... 2019Dokumen44 halamanUterine Cycle...... 2019Dina SartikaBelum ada peringkat
- Intrapartum NCM 107Dokumen8 halamanIntrapartum NCM 107Kimberly Sharah Mae FortunoBelum ada peringkat
- Obstetric NursingDokumen132 halamanObstetric NursingSteam LcBelum ada peringkat
- 2013 Maternal and Child Health Nursing Reviewer CompleteDokumen40 halaman2013 Maternal and Child Health Nursing Reviewer CompleteHarley Justiniani Dela CruzBelum ada peringkat
- Physiological Changes During 1st Stage of LaborDokumen18 halamanPhysiological Changes During 1st Stage of LaborNishaThakuri90% (39)
- Female Reproductive SystemDokumen17 halamanFemale Reproductive SystemShefali GoyalBelum ada peringkat
- Anatomy of Female ReproDokumen16 halamanAnatomy of Female ReproValarmathiBelum ada peringkat
- Presentation of Female Reproductive System. (Fallopian Tube)Dokumen11 halamanPresentation of Female Reproductive System. (Fallopian Tube)Nana Boakye IbrahimBelum ada peringkat
- Anatomy and Physiology of Female Reproductive System:: VaginaDokumen5 halamanAnatomy and Physiology of Female Reproductive System:: VaginaphallicBelum ada peringkat
- Obstetrics V10 Common Obstetric Conditions Chapter Pathology of The Placenta 1663285373Dokumen11 halamanObstetrics V10 Common Obstetric Conditions Chapter Pathology of The Placenta 1663285373Nurliana NingsihBelum ada peringkat
- Anatomy and Physiology GCSDokumen7 halamanAnatomy and Physiology GCSSherry Ann FayeBelum ada peringkat
- Pathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsDokumen35 halamanPathology of Pregnancy and Delivery: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielBelum ada peringkat
- 8 Bartholin's Glands: These Glands Are Located Next To The Vaginal Opening andDokumen4 halaman8 Bartholin's Glands: These Glands Are Located Next To The Vaginal Opening andalyssaaaaa1234885Belum ada peringkat
- Anatomy Physiology of Female Reproductive SystemDokumen96 halamanAnatomy Physiology of Female Reproductive SystemRabin BasnetBelum ada peringkat
- Case Pres TahbsoDokumen19 halamanCase Pres TahbsoHazel Endaya0% (1)
- Anatomy and PhysiologyDokumen8 halamanAnatomy and PhysiologyG3-PORTILLA John MartBelum ada peringkat
- Histo FemDokumen9 halamanHisto FemzaidBelum ada peringkat
- Anatomy and Physiology CASE STUDY (Final)Dokumen2 halamanAnatomy and Physiology CASE STUDY (Final)Glyndee Marr JagonobBelum ada peringkat
- Female Genital Tract and The Pelvic BonesDokumen37 halamanFemale Genital Tract and The Pelvic Bonesعبد الله الحربيBelum ada peringkat
- Uterus AnatomyDokumen7 halamanUterus AnatomyJoseph RadislaoBelum ada peringkat
- Breast: 1 EtymologyDokumen13 halamanBreast: 1 EtymologynathanBelum ada peringkat
- CP Ovarian Cyst Chap5Dokumen11 halamanCP Ovarian Cyst Chap5Katherine 'Chingboo' Leonico LaudBelum ada peringkat
- Intrapartum-EINC Integrated - 19Dokumen55 halamanIntrapartum-EINC Integrated - 19shannon c. lewisBelum ada peringkat
- UterusDokumen3 halamanUterusBernadette FlorendoBelum ada peringkat
- 1 - Mamary Gland Physiology and AnatomyDokumen12 halaman1 - Mamary Gland Physiology and Anatomym charan100% (1)
- Anatomy of Female Reproductive SystemDokumen7 halamanAnatomy of Female Reproductive SystemseongeokBelum ada peringkat
- Anatomy and Physiology: Functions of The UterusDokumen6 halamanAnatomy and Physiology: Functions of The UterusAnthony jesusBelum ada peringkat
- Anatomy and Physiology of OvaryDokumen2 halamanAnatomy and Physiology of OvaryFrancez Anne GuanzonBelum ada peringkat
- Female RSystemDokumen71 halamanFemale RSystemicliftonguytonBelum ada peringkat
- Documemt Fo ReprashingDokumen10 halamanDocumemt Fo ReprashingMarvellous OkonobohBelum ada peringkat
- Operative ReviewCSDokumen8 halamanOperative ReviewCSmarkie917Belum ada peringkat
- Effect of Kinesio Tape On Low Back Pain During Normal LaborDokumen28 halamanEffect of Kinesio Tape On Low Back Pain During Normal Laborj_______________j100% (3)
- Parts of The Reproductive OrganDokumen64 halamanParts of The Reproductive OrganFrancez Anne GuanzonBelum ada peringkat
- Anatomy and PhysiologyDokumen11 halamanAnatomy and PhysiologyJohn BretanaBelum ada peringkat
- Congenital Abnormalities of The UterusDokumen7 halamanCongenital Abnormalities of The Uterusمحمود الموسويBelum ada peringkat
- Case Study - CS With BTLDokumen16 halamanCase Study - CS With BTLAJ Roze Holmes100% (2)
- UNIT 11 (Reproductive System)Dokumen12 halamanUNIT 11 (Reproductive System)Workinesh Kaynabo KambaloBelum ada peringkat
- Ovarian Cyst FinalDokumen26 halamanOvarian Cyst FinalReicy Aquino SacularBelum ada peringkat
- Cow ReproductiveDokumen5 halamanCow Reproductiveastyrafe100% (1)
- Fix ObgynDokumen17 halamanFix ObgynDexter BluesBelum ada peringkat
- Maternal and Child Health Nursing ReviewerDokumen137 halamanMaternal and Child Health Nursing ReviewerDexie MaeBelum ada peringkat
- Family Case Study 1Dokumen12 halamanFamily Case Study 1Mark Anthony Torcino AbianBelum ada peringkat
- Reproductive SystemDokumen13 halamanReproductive SystemAlicia ValverdeBelum ada peringkat
- Female Reproductive SystemDokumen31 halamanFemale Reproductive SystemSusmita HalderBelum ada peringkat
- Anatomy & Physiology of Female Reproductive System: Dr. Aida Abd El-RazekDokumen96 halamanAnatomy & Physiology of Female Reproductive System: Dr. Aida Abd El-RazekJennifer DixonBelum ada peringkat
- Anatomical and Physiological Changes During PregnancyDokumen25 halamanAnatomical and Physiological Changes During Pregnancyqaleeq100% (1)
- Obstetric & Gynecology Nursing: Topic-Physiological Changes During LabourDokumen54 halamanObstetric & Gynecology Nursing: Topic-Physiological Changes During LabourBhumi ChouhanBelum ada peringkat
- Juanpablo Miguel ZAVALETA RODRIGUEZ - Human ReproductionDokumen23 halamanJuanpablo Miguel ZAVALETA RODRIGUEZ - Human ReproductionJuanpablo Miguel ZAVALETA RODRIGUEZBelum ada peringkat
- The Growing Fetus FertilizationDokumen6 halamanThe Growing Fetus FertilizationJustJ ThingsBelum ada peringkat
- Female Reproductive System, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandFemale Reproductive System, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Last Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsDari EverandLast Minute Embryology: Human embryology made easy and digestible for medical and nursing studentsBelum ada peringkat
- Jurnal Anak RirinDokumen10 halamanJurnal Anak RirinDexter BluesBelum ada peringkat
- Fix ObgynDokumen17 halamanFix ObgynDexter BluesBelum ada peringkat
- The Seven Cardinal MovementsDokumen4 halamanThe Seven Cardinal MovementsDexter BluesBelum ada peringkat
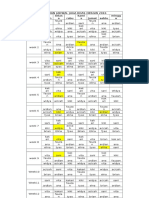
- Rincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDokumen1 halamanRincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDexter BluesBelum ada peringkat
- 1830 PDF PDFDokumen5 halaman1830 PDF PDFDexter BluesBelum ada peringkat
- Ngeo2472 s1 PDFDokumen4 halamanNgeo2472 s1 PDFDexter BluesBelum ada peringkat
- UlnarClubHandweb PDFDokumen2 halamanUlnarClubHandweb PDFDexter BluesBelum ada peringkat
- Statement On STERRAD NX Sterilization of Richard Wolf Medical Devices-EnDokumen3 halamanStatement On STERRAD NX Sterilization of Richard Wolf Medical Devices-EnmarjuniBelum ada peringkat
- Chapter 3 Daily Life of The Colonies Housekeeping, Children, and SexDokumen6 halamanChapter 3 Daily Life of The Colonies Housekeeping, Children, and SexlagurrBelum ada peringkat
- Ethicon STEPS Advert 2020Dokumen1 halamanEthicon STEPS Advert 2020vlad910Belum ada peringkat
- Ricucci-2011: Outcome Study For EndodonticsDokumen18 halamanRicucci-2011: Outcome Study For EndodonticsKristineBelum ada peringkat
- G HDPDokumen32 halamanG HDPkunkkonkBelum ada peringkat
- Operation Theatre ManagementDokumen55 halamanOperation Theatre ManagementSushmitaBhaumik100% (73)
- Asian Rhinoplasty (Noselift) - Cosmetic Surgery in The PhilippinesDokumen1 halamanAsian Rhinoplasty (Noselift) - Cosmetic Surgery in The Philippinesdalemd29Belum ada peringkat
- Level 0 Diagram: Registered Patient New PatientDokumen2 halamanLevel 0 Diagram: Registered Patient New PatientShaira BugayongBelum ada peringkat
- Apex HospitalDokumen33 halamanApex HospitalRaj PalBelum ada peringkat
- CapsulotomyDokumen15 halamanCapsulotomyAdrian PearlBelum ada peringkat
- A Brief On MGRM MedicareDokumen2 halamanA Brief On MGRM MedicareSai Kishore KBelum ada peringkat
- Government College of Nursing Jodhpur (Raj.)Dokumen5 halamanGovernment College of Nursing Jodhpur (Raj.)priyanka100% (1)
- JADWAL PRAKTEK DOKTER RSMK BKS Barat JUNI REVISI 2022Dokumen2 halamanJADWAL PRAKTEK DOKTER RSMK BKS Barat JUNI REVISI 2022soegi2012Belum ada peringkat
- The Cox-Maze IV Procedure For Lone Atrial Fibrillation - A Single Center Experience in 100 Consecutive Patients.Dokumen2 halamanThe Cox-Maze IV Procedure For Lone Atrial Fibrillation - A Single Center Experience in 100 Consecutive Patients.Juan Diego RestrepoBelum ada peringkat
- Radiology Developing Technique ChartsDokumen4 halamanRadiology Developing Technique ChartsVarghese NellimoottilBelum ada peringkat
- VawpregnancyDokumen2 halamanVawpregnancyOkto 'Andri' SaputraBelum ada peringkat
- Resume Ebrahim RadinniaDokumen2 halamanResume Ebrahim RadinniaSepideh MirzaeiBelum ada peringkat
- Kanker Ovarium 2 PDFDokumen6 halamanKanker Ovarium 2 PDFhestiBelum ada peringkat
- Male InfertilityDokumen63 halamanMale InfertilitySuhaila SabanBelum ada peringkat
- POST-TEST Mock Written Diplomate ExaminationDokumen62 halamanPOST-TEST Mock Written Diplomate ExaminationRem AlfelorBelum ada peringkat
- Eye Banking OphthalmologyDokumen21 halamanEye Banking Ophthalmologyvivekrajbhilai5850100% (2)
- Hospital OrientationDokumen82 halamanHospital OrientationDondee Pamposa100% (2)
- Effectiveness of Pelvic Bridge Exercise On Dysmenorrhea - Thesis PDFDokumen149 halamanEffectiveness of Pelvic Bridge Exercise On Dysmenorrhea - Thesis PDFAruna G100% (1)
- Which Local Anesthesia Application Should We Use During Circumcision?Dokumen2 halamanWhich Local Anesthesia Application Should We Use During Circumcision?asclepiuspdfsBelum ada peringkat
- CH 6 Part 1Dokumen7 halamanCH 6 Part 1ArenBelum ada peringkat
- MCQ On Menstrual CycleDokumen7 halamanMCQ On Menstrual CycleKarishma Shroff100% (2)
- ECG Interpretations DR RPDokumen109 halamanECG Interpretations DR RPArnis Putri RosyaniBelum ada peringkat
- Data Publikasi Artikel Ilmiah Penelitian Dan Pengabmas Kebidanan FixDokumen9 halamanData Publikasi Artikel Ilmiah Penelitian Dan Pengabmas Kebidanan FixMuhamad Vanny OntaluBelum ada peringkat
- Nursing Role of Cardiac and Respiratory Arrest Checklist 2022 ApproveDokumen3 halamanNursing Role of Cardiac and Respiratory Arrest Checklist 2022 ApproveDo0odi AlharbiBelum ada peringkat
- Admision FormDokumen8 halamanAdmision FormRyles ZenegadeBelum ada peringkat