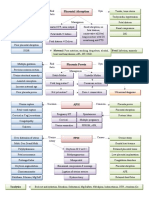
Accurate method of estimating
thyroid function compensates for
GFR Iodine by 50%
Free T4 conc. Thyroid Function Pregnanc
test THYROID DISEASE y
Serum bound T3 and T4
Iodide (freely cross placenta)
Freely
Cross Placent <10 w no iodine in
TSH-Ab (cause fetal thyroid al
thyroid
Transf 11 to 12 w produce T4
Fetal Thyroid
T4 (important for neural Function
development in first trimester >12 w Able to concentrate
Limit
before mature fetal thyroid) ed iodine, and Fetal TSH, T4,
TRH (low circ. levels, not and free T4 mature thyroid
TSH (DOES NOT CROSS) Do Not
Cross
Prematurity Complicati Maternal Hyperthyroidism Incidence 1 per 500
ons pregnancies
IUGR Graves’ disease (most)
Investigatio Treatment
Sympto
ns
Superimposed PET ms
Difficult (many S&S are
Serum free T4 Propylthiouracil (PUT) &
Stillbirth present in normal euthyroid
Methimazole cross
pregnancies)
Neonatal M&M TSH levels placenta (can cause fetal Resting pulse > 100 bpm
hypothyroidism) give (fails to slow with Valsalva
Precipitating minimal dose for within maneuver)
Thyroid Storm factors Radioactive iodine Rx Eye changes, Weight loss,
S&S Heat intolerance
Infection
Surgical Rx only if Medical fails
Hyperthermia Labor
Marked tachycardia Cesarean
Perspiration Noncompliance Maternal Hypothyroidism
Complicati
High output failure Investigati
Treatment on ons
Severe dehydration Spontaneous Abortion
TSH levels (imp)
Propanolol
PET
Neonatal Sodium iodide Neonatal
Abruption
PTU
1% (due to TSH-Ab Congenital Hypothyroidism LBW/Stillbirth
Dexamethesone
Lasts 2 – 3 months Generalized Developmental Lower IQ (cretinism)
Fluid replacement
16% neonatal mortality Etiology: thyroid dysgenesis, inborn
Hypothermic
Fetal HR continently > Most common cause of neonatal goiter
Fetal goiter seen on US is maternal ingestion of iodideds
present in cough syrup
Anda mungkin juga menyukai
- Lecture 29 30 Thyroid TherapeuticsDokumen3 halamanLecture 29 30 Thyroid TherapeuticsAhmed MashalyBelum ada peringkat
- PDFDokumen70 halamanPDFPaul Benjomin AgregadoBelum ada peringkat
- 3 Treatment of HypertensionDokumen7 halaman3 Treatment of HypertensiontiaraBelum ada peringkat
- Chief Complaint FormatDokumen3 halamanChief Complaint Formatkazniels100% (1)
- Internal Medicine #1Dokumen167 halamanInternal Medicine #1Nikhil RayarakulaBelum ada peringkat
- Trusted Evidence For Confident Clinical Decisions: Resources For Medication, Disease, and ToxicologyDokumen10 halamanTrusted Evidence For Confident Clinical Decisions: Resources For Medication, Disease, and ToxicologyCurcubeuAuroraBelum ada peringkat
- Alarm Symptoms of Hematoonco in Pediatrics: Dr. Cece Alfalah, M.Biomed, Sp.A (K) Pediatric Hematology and OncologyDokumen22 halamanAlarm Symptoms of Hematoonco in Pediatrics: Dr. Cece Alfalah, M.Biomed, Sp.A (K) Pediatric Hematology and OncologyMuhammad ArifBelum ada peringkat
- Pharm Fall Cardiovascular Pharmacology Study Guide-106Dokumen47 halamanPharm Fall Cardiovascular Pharmacology Study Guide-106sean liyanageBelum ada peringkat
- Diagnosis and Treatment of Bacterial ProstatitisDokumen5 halamanDiagnosis and Treatment of Bacterial ProstatitislobeseyBelum ada peringkat
- Antiphospholipid Syndrome (Aps) and PregnancyDokumen36 halamanAntiphospholipid Syndrome (Aps) and Pregnancyskeisham11Belum ada peringkat
- Mo Intern Handbook - FinalDokumen37 halamanMo Intern Handbook - FinalGideon K. MutaiBelum ada peringkat
- Abx FinalDokumen3 halamanAbx Finalyanks1120Belum ada peringkat
- Physiology Clinical Diagnosis Treatment: TSI AntibodiesDokumen10 halamanPhysiology Clinical Diagnosis Treatment: TSI Antibodies85robertBelum ada peringkat
- Pneumonia Cheat Sheet: by ViaDokumen3 halamanPneumonia Cheat Sheet: by ViaGayle MarieBelum ada peringkat
- STEP 1 ChecklistDokumen11 halamanSTEP 1 ChecklistHasan Khan RoudbaryBelum ada peringkat
- Post-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetDokumen3 halamanPost-Cardiac Arrest Therapeutic Hypothermia Targeted Temperature Manangement (TTM) Quick SheetkimberlyBelum ada peringkat
- Thrombocytopenia in PregnancyDokumen13 halamanThrombocytopenia in PregnancyJhuli Elizabeth CBelum ada peringkat
- Normal Lab Values (USMLE Step 1)Dokumen12 halamanNormal Lab Values (USMLE Step 1)nmp274Belum ada peringkat
- Personal Statement - FinalDokumen2 halamanPersonal Statement - Finalapi-383932502Belum ada peringkat
- Gastroenterology AscitesDokumen2 halamanGastroenterology AscitesNour SamadBelum ada peringkat
- Helminth ChartsDokumen4 halamanHelminth ChartsDrbee10Belum ada peringkat
- Epidemiology 2Dokumen15 halamanEpidemiology 2Rozen Tareque HasanBelum ada peringkat
- Mood Disorders: Advanced Practice Education AssociatesDokumen11 halamanMood Disorders: Advanced Practice Education AssociatesAndrea100% (1)
- USMLE Step 2 CK 6 Months Study Plan For 240Dokumen1 halamanUSMLE Step 2 CK 6 Months Study Plan For 240DhritisdiaryBelum ada peringkat
- 08&09 Oral Hypoglycemics-Level 11Dokumen48 halaman08&09 Oral Hypoglycemics-Level 11Usman Ali AkbarBelum ada peringkat
- Antiarrhythmic Drugs: More To Inactivated Na Channels Arrhythmias During Myocardial Ischaemia or Due To DigoxinDokumen3 halamanAntiarrhythmic Drugs: More To Inactivated Na Channels Arrhythmias During Myocardial Ischaemia or Due To DigoxinChia Yin NgBelum ada peringkat
- Pharm - Chapter - 13 - Central Nervous System StimulantsDokumen42 halamanPharm - Chapter - 13 - Central Nervous System StimulantsFeliciaDorghamBelum ada peringkat
- Drug Toxicity and PoisoningDokumen12 halamanDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDOBelum ada peringkat
- Slides of Fever 3Dokumen52 halamanSlides of Fever 3Selly SelBelum ada peringkat
- Autoimmune Diseases: Henry O. Ogedegbe, PHD., C (Ascp) SC Department of EhmcsDokumen47 halamanAutoimmune Diseases: Henry O. Ogedegbe, PHD., C (Ascp) SC Department of EhmcsGalih Putra RanggaBelum ada peringkat
- INITIAL PRENATAL ASSESSMENT ProcedureDokumen17 halamanINITIAL PRENATAL ASSESSMENT ProcedureCyndryl SampotonBelum ada peringkat
- 5 6231116747487838836Dokumen466 halaman5 6231116747487838836Indah Siti SopiahBelum ada peringkat
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDokumen1 halamanGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentMuthia ArsilBelum ada peringkat
- H&PEDokumen2 halamanH&PEDanielleBelum ada peringkat
- Step1 Review TopicsDokumen32 halamanStep1 Review TopicsAsif AbidiBelum ada peringkat
- Sudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015Dokumen23 halamanSudden Maternal Collapse: Max Brinsmead MB Bs PHD May 2015DrChauhanBelum ada peringkat
- Diabetes and Complications: When Documenting Diabetes, It's Important To Note The FollowingDokumen2 halamanDiabetes and Complications: When Documenting Diabetes, It's Important To Note The Followingmeikaizen100% (1)
- Approach To Hematuria and Proteinuria in ChildrenDokumen52 halamanApproach To Hematuria and Proteinuria in ChildrenMysheb SS100% (1)
- Management of Common Cases in Emergency MedicineDokumen55 halamanManagement of Common Cases in Emergency MedicinemonpyitharBelum ada peringkat
- Practice Problems CH 5Dokumen15 halamanPractice Problems CH 5rehassan100% (2)
- How Do I Diagnose The Cause of A Cough of Less Than 3 Weeks' Duration?Dokumen14 halamanHow Do I Diagnose The Cause of A Cough of Less Than 3 Weeks' Duration?Sudhir TyagiBelum ada peringkat
- Article - Medical ErrorsDokumen4 halamanArticle - Medical ErrorsDavid S. ChouBelum ada peringkat
- Enteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsDokumen14 halamanEnteral Versus Parenteral Nutrition in Critically Ill Patients - An Updated Systematic Review and Meta-Analysis of Randomized Controlled TrialsLea Bali Ulina SinurayaBelum ada peringkat
- Fall Risk Assessment Form: Total Score - A Total Score of 10 or More Indicates A Resident "At Risk" For FallsDokumen1 halamanFall Risk Assessment Form: Total Score - A Total Score of 10 or More Indicates A Resident "At Risk" For FallswaheedmohsinBelum ada peringkat
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDokumen25 halamanClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiBelum ada peringkat
- With Dr. Susan Lipsett: Community Acquired PneumoniaDokumen1 halamanWith Dr. Susan Lipsett: Community Acquired PneumoniaJayantiBelum ada peringkat
- Meds Affecting Reproduction: (General Key Points)Dokumen20 halamanMeds Affecting Reproduction: (General Key Points)susan2johnson-501300Belum ada peringkat
- Chemical Pathology Reference Range 2017Dokumen19 halamanChemical Pathology Reference Range 2017Shobana RaveendranBelum ada peringkat
- (Pedia 3A) NEPHRO COMPILED PDFDokumen40 halaman(Pedia 3A) NEPHRO COMPILED PDFNoreenBelum ada peringkat
- Weekly Clinical Prep Packet 12 REVISEDDokumen12 halamanWeekly Clinical Prep Packet 12 REVISEDMei SarteBelum ada peringkat
- Pathophysiology 2Dokumen92 halamanPathophysiology 2Princess AgarwalBelum ada peringkat
- Deconstructing The ECG Curve - The Components of The Tracing: Key ConceptsDokumen117 halamanDeconstructing The ECG Curve - The Components of The Tracing: Key ConceptsdrynwhylBelum ada peringkat
- 10 Pharmacology - ImmunopharmacologyDokumen17 halaman10 Pharmacology - ImmunopharmacologyArnoldBorromeoBelum ada peringkat
- Analysis of Heart Sounds and Murmurs by Digital Signal ManipulationDokumen95 halamanAnalysis of Heart Sounds and Murmurs by Digital Signal ManipulationFerdayBelum ada peringkat
- Venous DisDokumen41 halamanVenous DisAdel SalehBelum ada peringkat
- C 21Dokumen23 halamanC 21jackBelum ada peringkat
- Chemotherapy and Biotherapy Hypersensitivity Reactions: Christine E. Coyle, RN, BSN, OCNDokumen55 halamanChemotherapy and Biotherapy Hypersensitivity Reactions: Christine E. Coyle, RN, BSN, OCNRakesh MishraBelum ada peringkat
- Allergic Rhinitis - University of MichiganDokumen12 halamanAllergic Rhinitis - University of MichiganarsyiadlinaBelum ada peringkat
- 14 - Toronto Notes 2011 - GynecologyDokumen52 halaman14 - Toronto Notes 2011 - GynecologyZiyad100% (4)
- Fluid Management in PediatricsDokumen3 halamanFluid Management in PediatricsZiyadBelum ada peringkat
- Acyanotic Congenital Heart DiseaseDokumen2 halamanAcyanotic Congenital Heart DiseaseZiyad100% (1)
- EndometriosisDokumen1 halamanEndometriosisZiyad100% (1)
- Instruments & IndicationsDokumen11 halamanInstruments & IndicationsZiyad100% (2)
- Obstetric BleedingDokumen1 halamanObstetric BleedingZiyadBelum ada peringkat
- Urinary IncontinenceDokumen1 halamanUrinary IncontinenceZiyad100% (1)
- BreechDokumen1 halamanBreechZiyadBelum ada peringkat
- Human Nutrition: (Iodine, Fluoride, Magnesium)Dokumen37 halamanHuman Nutrition: (Iodine, Fluoride, Magnesium)CancerBelum ada peringkat
- Advanced TUS 2017 Syllabus - SECUREDDokumen373 halamanAdvanced TUS 2017 Syllabus - SECUREDYav KBelum ada peringkat
- (Self-Assessment Color Review) Joyce E. Obradovich - Small Animal Clinical Oncology - Self-Assessment Color review-CRC Press (2017)Dokumen329 halaman(Self-Assessment Color Review) Joyce E. Obradovich - Small Animal Clinical Oncology - Self-Assessment Color review-CRC Press (2017)dpcamposhBelum ada peringkat
- Tips Current Procedures SurgeryDokumen844 halamanTips Current Procedures SurgeryMersed HuremovicBelum ada peringkat
- Isfm HipertiroidismoDokumen17 halamanIsfm HipertiroidismoMaria Rodriguez RodrguezBelum ada peringkat
- Review Cram SheetDokumen57 halamanReview Cram Sheetjim j100% (1)
- A&p - All Files in One PDFDokumen52 halamanA&p - All Files in One PDFSreejith Jagal KishoreBelum ada peringkat
- Thyroid Function TestingDokumen12 halamanThyroid Function TestingDewi Paramita YuniarahmiBelum ada peringkat
- Big Testicles Ebook PDFDokumen73 halamanBig Testicles Ebook PDFCamillo Granata64% (11)
- Psychology Mcq'sDokumen4 halamanPsychology Mcq'sMuhammad IkramBelum ada peringkat
- Station 5 Example ScenariosDokumen5 halamanStation 5 Example ScenariosGajanan GuptaBelum ada peringkat
- Ref Ultrasoud of The Normal Thyroid 2020Dokumen7 halamanRef Ultrasoud of The Normal Thyroid 2020Daniel Alejandro CastrilloBelum ada peringkat
- 07122022am326c71270060893425 RLSDokumen2 halaman07122022am326c71270060893425 RLSPt computerBelum ada peringkat
- Product Preview i-CHROMA Boditech PDFDokumen25 halamanProduct Preview i-CHROMA Boditech PDFUMARALEKSANA, CV100% (2)
- Dr. Osama Mahmoud (Endocrinology)Dokumen253 halamanDr. Osama Mahmoud (Endocrinology)Mohammad Abd-AlhafezBelum ada peringkat
- Droste 2007Dokumen4 halamanDroste 2007Aisyah DewiBelum ada peringkat
- Endocrinology Notes: Veterinary PhysiologyDokumen16 halamanEndocrinology Notes: Veterinary PhysiologyBrian AllanBelum ada peringkat
- MCQ Bank PDFDokumen38 halamanMCQ Bank PDFShafiq Ur Rahman100% (1)
- Anasurgery MockboardDokumen12 halamanAnasurgery MockboardVince CabahugBelum ada peringkat
- Subclinical Thyroid DiseaseDokumen50 halamanSubclinical Thyroid Diseaseกรคุง ภิญโญพจนารถBelum ada peringkat
- Endocrinology LastDokumen44 halamanEndocrinology Lastlestrange1984100% (1)
- Endocrine Disorders Julie Mann, NP - Case StudyDokumen10 halamanEndocrine Disorders Julie Mann, NP - Case Studysimonedarling75% (4)
- MCNP Integrated Concepts NP 3Dokumen9 halamanMCNP Integrated Concepts NP 3Karen Mae Santiago AlcantaraBelum ada peringkat
- HipertiroidDokumen96 halamanHipertiroidOja KarnilaBelum ada peringkat
- The Dangers of Quitting SugarDokumen9 halamanThe Dangers of Quitting Sugarsimx88100% (2)
- Csec Biology TestDokumen8 halamanCsec Biology TestImmanuel LashleyBelum ada peringkat
- SC2 2015 HyperthyroidismDokumen38 halamanSC2 2015 HyperthyroidismShafern TanBelum ada peringkat
- Mockboards Reviewer FinalDokumen161 halamanMockboards Reviewer FinalRoselle Joyce Arce CalubanBelum ada peringkat
- anti-TPO (aTPO) : Assay For The Detection of Autoantibodies Against Thyroid PeroxidaseDokumen10 halamananti-TPO (aTPO) : Assay For The Detection of Autoantibodies Against Thyroid PeroxidaseGuneyden GuneydenBelum ada peringkat
- Beta HCG: Test Result Units Reference IntervalDokumen3 halamanBeta HCG: Test Result Units Reference IntervalBALABelum ada peringkat