Anda mungkin juga menyukai
- Central Venous AccessDokumen21 halamanCentral Venous AccessChrisBelum ada peringkat
- Surgical ApproachDokumen124 halamanSurgical ApproachHendra AjahBelum ada peringkat
- Venous and Arterial Catheterization: General PrinciplesDokumen22 halamanVenous and Arterial Catheterization: General PrinciplesTibin JosephBelum ada peringkat
- Anterolateral Approach of Proximal Humerus + Henry ApproachDokumen33 halamanAnterolateral Approach of Proximal Humerus + Henry ApproachwildanmalikBelum ada peringkat
- Anesthesia of The Lower Alveolar NerveDokumen44 halamanAnesthesia of The Lower Alveolar Nerve陳碩璠Belum ada peringkat
- Ao Pedicle ScrewDokumen3 halamanAo Pedicle ScrewPramod N KBelum ada peringkat
- (Ii) Surgical Approaches To The Knee Joint: Anteromedial Parapatellar ApproachDokumen8 halaman(Ii) Surgical Approaches To The Knee Joint: Anteromedial Parapatellar ApproachDaniel G. A. C.Belum ada peringkat
- Surgical Approaches To TMJDokumen39 halamanSurgical Approaches To TMJachukrishna2Belum ada peringkat
- Surgical Approaches To The Facial Skeleton Mandible and TMJDokumen24 halamanSurgical Approaches To The Facial Skeleton Mandible and TMJRagavi VijayaragavanBelum ada peringkat
- H&N - Cervical Plexus BlockDokumen9 halamanH&N - Cervical Plexus BlockJane KoBelum ada peringkat
- NYSORA Thoracic Paravertebral BlockDokumen16 halamanNYSORA Thoracic Paravertebral BlockYee Yeow100% (1)
- Art HR OgraphyDokumen60 halamanArt HR OgraphyBikash SubediBelum ada peringkat
- Thoracic & Abdominal Wall BlocksDokumen57 halamanThoracic & Abdominal Wall Blocksvignoth23112000Belum ada peringkat
- Umbilical Artery CatheterizationDokumen9 halamanUmbilical Artery CatheterizationrohitBelum ada peringkat
- Cannulation of The Internal Jugular Vein: Robert Cambria, MDDokumen9 halamanCannulation of The Internal Jugular Vein: Robert Cambria, MDAndres BernalBelum ada peringkat
- Mamiek Dwi Putro Departemen / SMF Ilmu Bedah FK Unair / RSU DR Soetomo SurabayaDokumen38 halamanMamiek Dwi Putro Departemen / SMF Ilmu Bedah FK Unair / RSU DR Soetomo SurabayamasmblinkBelum ada peringkat
- Cervical Plexus BlocksDokumen57 halamanCervical Plexus Blocksnorociel8132Belum ada peringkat
- Types of IncisionsDokumen6 halamanTypes of IncisionsKim GomezBelum ada peringkat
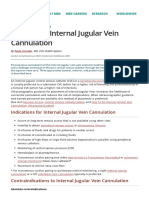
- How To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionDokumen9 halamanHow To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionnaveenBelum ada peringkat
- Epidural AnesthesiaDokumen32 halamanEpidural AnesthesiaAmareBelum ada peringkat
- Supraclavicular Block: Arthur Atchabahian, MDDokumen4 halamanSupraclavicular Block: Arthur Atchabahian, MDAli AftabBelum ada peringkat
- Regional Anesthesia: Brachial Plexus BlockDokumen77 halamanRegional Anesthesia: Brachial Plexus BlockTerefe AlemayehuBelum ada peringkat
- Inferior Alveolar TechniqueDokumen8 halamanInferior Alveolar Techniquebalab2311Belum ada peringkat
- Surgical Approaches To Shoulder Joint - 075527Dokumen32 halamanSurgical Approaches To Shoulder Joint - 075527nihal adriel gomesBelum ada peringkat
- Regional Anesthesia: Dr. Wasim R. IssaDokumen37 halamanRegional Anesthesia: Dr. Wasim R. IssaWasim R. IssaBelum ada peringkat
- Tracheostomy PDFDokumen8 halamanTracheostomy PDFVeronica GaticaBelum ada peringkat
- Rhinoplasty WorkbookDokumen21 halamanRhinoplasty Workbookzena talibBelum ada peringkat
- Vertebroplasty: DR Eslam Mohmad Abd El-Ghaffar Ahmed Maher Teaching HospitalDokumen14 halamanVertebroplasty: DR Eslam Mohmad Abd El-Ghaffar Ahmed Maher Teaching Hospitalamae85Belum ada peringkat
- THR Surgical ApproachesDokumen5 halamanTHR Surgical ApproachesMaria Magdalena SmeuBelum ada peringkat
- Stellate Ganglion Block by Dr. JayDokumen32 halamanStellate Ganglion Block by Dr. JayDr Jay Panchal100% (2)
- Surface Anatomy and Other LandmarksDokumen7 halamanSurface Anatomy and Other LandmarksoristoBelum ada peringkat
- Traditional Approaches To The OrbitDokumen15 halamanTraditional Approaches To The Orbitapi-19500641Belum ada peringkat
- Surgical Approaches ElbowDokumen68 halamanSurgical Approaches ElbowPrakash AyyaduraiBelum ada peringkat
- Surgical Incision Head & NeckDokumen31 halamanSurgical Incision Head & Neckromzikerenz0% (1)
- Approaches To Distal FemurDokumen23 halamanApproaches To Distal FemursanjudnlBelum ada peringkat
- Section Iic Suturing Techniques 2015Dokumen13 halamanSection Iic Suturing Techniques 2015André Pinheiro de AraújoBelum ada peringkat
- Surgical Approaches To The Facial Skeleton: Mandible and TMJDokumen141 halamanSurgical Approaches To The Facial Skeleton: Mandible and TMJRagavi Vijayaragavan100% (1)
- Deltopectoral ApproachDokumen4 halamanDeltopectoral ApproachAlex DiconiBelum ada peringkat
- Rectal CancerDokumen20 halamanRectal CancerSantosh BabuBelum ada peringkat
- Triple ArthrodesisDokumen10 halamanTriple ArthrodesisdrkbarryBelum ada peringkat
- Middle FossaDokumen16 halamanMiddle FossaSebastianBelum ada peringkat
- Central Venous LinesDokumen34 halamanCentral Venous LinesManny TrujilloBelum ada peringkat
- Group 4 - Types of Incision, and Post Operative ComplicationsDokumen21 halamanGroup 4 - Types of Incision, and Post Operative ComplicationsGeraldine GodesBelum ada peringkat
- Anatomy of The AxillarDokumen43 halamanAnatomy of The AxillarJustine NyangaresiBelum ada peringkat
- Esofagostomia CervicalaDokumen11 halamanEsofagostomia CervicalaRoxa777Belum ada peringkat
- Closing TechniquesDokumen14 halamanClosing TechniquesAndrei BulgariuBelum ada peringkat
- Critical Care ProtocolsDokumen19 halamanCritical Care ProtocolsPrabhat KumarBelum ada peringkat
- OB Hemorrhage ADJUNCT SURGICAL PROCEDURESDokumen3 halamanOB Hemorrhage ADJUNCT SURGICAL PROCEDURESRTP3 Angeli SalutBelum ada peringkat
- Chest Tube InsertionDokumen4 halamanChest Tube InsertionHugo ARBelum ada peringkat
- Intracranial TensionDokumen14 halamanIntracranial Tensionpemetaan dokumen aktreditasi100% (1)
- IM Injections Clinical TechsadaniqueDokumen2 halamanIM Injections Clinical TechsadaniqueGeminiQueenBelum ada peringkat
- GluteusDokumen4 halamanGluteuskoxBelum ada peringkat
- Central Venous CatheterizationDokumen20 halamanCentral Venous Catheterizationdrhiwaomer100% (3)
- Arteries of Head and NeckDokumen77 halamanArteries of Head and NeckdeepthamagetBelum ada peringkat
- Ankle AnatomyDokumen50 halamanAnkle AnatomyLiao WangBelum ada peringkat
- Abdominal Region Part 2Dokumen58 halamanAbdominal Region Part 2Swati LataBelum ada peringkat
- Access Vascular FOR Hemodialysis: Dr. Sahal Fatah, SP - BTKVDokumen28 halamanAccess Vascular FOR Hemodialysis: Dr. Sahal Fatah, SP - BTKVAnonymous wVgEAr6Belum ada peringkat
- Cervical Epidural Steroid Injection: DR A Sugeng Wibisono, Span, Fipm, FippDokumen49 halamanCervical Epidural Steroid Injection: DR A Sugeng Wibisono, Span, Fipm, FippAndari SetianingtyasBelum ada peringkat
- Acr Eular Clasificacion ArDokumen12 halamanAcr Eular Clasificacion ArAnghelo Aldair Velásquez CarrilloBelum ada peringkat
- Bol 2Dokumen1 halamanBol 2Julio CamachoBelum ada peringkat
- A-Z of Emergency RadiologyDokumen178 halamanA-Z of Emergency RadiologyIamandi Cristina100% (1)
- Therapy of Diffuse or Focal Proliferative Lupus Nephritis - UpToDateDokumen28 halamanTherapy of Diffuse or Focal Proliferative Lupus Nephritis - UpToDateJulio Camacho100% (1)
- Eula Microsoft Visual StudioDokumen3 halamanEula Microsoft Visual StudioqwwerttyyBelum ada peringkat
- Neurological Physiotherapy Evaluation Form 2 0Dokumen82 halamanNeurological Physiotherapy Evaluation Form 2 0Eman SabryBelum ada peringkat
- ACS/ASE Medical Student Core Curriculum Trauma II: Diagnosis and ManagementDokumen35 halamanACS/ASE Medical Student Core Curriculum Trauma II: Diagnosis and ManagementJefriantoBelum ada peringkat
- Douglas Freeman AutopsyDokumen7 halamanDouglas Freeman Autopsyreef_galBelum ada peringkat
- The Minipterional Craniotomy For Anterior.5Dokumen8 halamanThe Minipterional Craniotomy For Anterior.5J Alan SantosBelum ada peringkat
- Lesson 2.1 Instructor NotesDokumen6 halamanLesson 2.1 Instructor NotesCaleb FlaxBelum ada peringkat
- Limba LatinaDokumen2 halamanLimba LatinaAlina AlinaBelum ada peringkat
- Mcqs Babu S ParmerDokumen320 halamanMcqs Babu S Parmershoaibiidc8Belum ada peringkat
- Ascad Asit For AnimalsDokumen87 halamanAscad Asit For AnimalsThamil Arasan100% (1)
- Dental Anatomy Notes PDFDokumen27 halamanDental Anatomy Notes PDFJonathanBelum ada peringkat
- 7 0 Student WorkbookDokumen17 halaman7 0 Student Workbookapi-343368893Belum ada peringkat
- 78338-Anatomy of The Oral Cavity Pharynx and Larynx - SchuknechtDokumen6 halaman78338-Anatomy of The Oral Cavity Pharynx and Larynx - SchuknechtvldBelum ada peringkat
- Bleeding After TonsillectomyDokumen7 halamanBleeding After Tonsillectomyking_petarBelum ada peringkat
- 3) Thyroid Gland MDSC 2101 2014Dokumen32 halaman3) Thyroid Gland MDSC 2101 2014Kay Bristol100% (1)
- Embryology of Heart Year 2Dokumen55 halamanEmbryology of Heart Year 2Amanuel MaruBelum ada peringkat
- IVMS ICM-Heart MurmursDokumen22 halamanIVMS ICM-Heart MurmursMarc Imhotep Cray, M.D.Belum ada peringkat
- ENT McqsDokumen21 halamanENT McqsDr.G.Bhanu Prakash100% (8)
- Final LMRDokumen118 halamanFinal LMRPrabhat KcBelum ada peringkat
- Reviewer For Zoology LabDokumen18 halamanReviewer For Zoology LabayeyedumpBelum ada peringkat
- 5b9f87df82236UG Syllabus (MBBS) AIIMS RaipurDokumen8 halaman5b9f87df82236UG Syllabus (MBBS) AIIMS RaipurBri MinBelum ada peringkat
- Clinical Anatomy NotesDokumen5 halamanClinical Anatomy NotesYehansa WijethungaBelum ada peringkat
- Second FridayDokumen6 halamanSecond FridaymrashaiedehBelum ada peringkat
- Penetrating Neck Injuries - Initial Evaluation and Management - UpToDateDokumen20 halamanPenetrating Neck Injuries - Initial Evaluation and Management - UpToDateVerónica VidalBelum ada peringkat
- FILE - 20191227 - 140801 - 4. Đề-thi-HKI-avcn K43Dokumen8 halamanFILE - 20191227 - 140801 - 4. Đề-thi-HKI-avcn K43Liễu PhươngBelum ada peringkat
- DissectionManual-Book - XXXX PDFDokumen190 halamanDissectionManual-Book - XXXX PDFHossam Thabet100% (2)
- Bocca Functional Neck DissectionDokumen4 halamanBocca Functional Neck DissectionNoma OlomuBelum ada peringkat
- Anatomy of The Face and Neck: Peter M. PrendergastDokumen18 halamanAnatomy of The Face and Neck: Peter M. PrendergastMaher Khoury100% (1)
- IndianJRadiolImaging - Imaging in Laringeal CancerDokumen18 halamanIndianJRadiolImaging - Imaging in Laringeal CancerMirela IordacheBelum ada peringkat
- Anesthesia For Carotid EndarterectomyDokumen89 halamanAnesthesia For Carotid EndarterectomyChavdarBelum ada peringkat
- A General-Purpose Color Doppler Ultrasound SystemDokumen15 halamanA General-Purpose Color Doppler Ultrasound SystemMaged BedeawyBelum ada peringkat
- Dissection of A Fetal PigDokumen36 halamanDissection of A Fetal PigMadhu JohnBelum ada peringkat
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (81)
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 4 dari 5 bintang4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDari EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDPenilaian: 5 dari 5 bintang5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePenilaian: 2 dari 5 bintang2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (26)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDari EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (42)
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsPenilaian: 5 dari 5 bintang5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDari EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsBelum ada peringkat
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 4 dari 5 bintang4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDari EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryPenilaian: 4 dari 5 bintang4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerDari EverandGut: the new and revised Sunday Times bestsellerPenilaian: 4 dari 5 bintang4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDari EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- The Marshmallow Test: Mastering Self-ControlDari EverandThe Marshmallow Test: Mastering Self-ControlPenilaian: 4.5 dari 5 bintang4.5/5 (58)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDari EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingPenilaian: 4 dari 5 bintang4/5 (1138)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDari EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningPenilaian: 4 dari 5 bintang4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (170)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDari EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (328)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsDari EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsPenilaian: 4.5 dari 5 bintang4.5/5 (6)