Anda mungkin juga menyukai
- 4th Grade Reading Comprehension 5Dokumen0 halaman4th Grade Reading Comprehension 5Joy Hyun Seung LeeBelum ada peringkat
- Approach To Poisoned PatientDokumen90 halamanApproach To Poisoned PatientGopi KrishnanBelum ada peringkat
- The Mitchell Method of Physiological Relaxation: - A Simple Technique Suitable For AllDokumen12 halamanThe Mitchell Method of Physiological Relaxation: - A Simple Technique Suitable For AllGopi KrishnanBelum ada peringkat
- Lesson Plan For SpeedDokumen2 halamanLesson Plan For SpeedJonard Pacres AbrasadoBelum ada peringkat
- NeurosurgeryDokumen9 halamanNeurosurgeryGopi KrishnanBelum ada peringkat
- Fundamentals of Insight Meditation - Mahasi Sayadaw-1959Dokumen56 halamanFundamentals of Insight Meditation - Mahasi Sayadaw-1959BuddhaDhammaSangahBelum ada peringkat
- Psychosomatic Means Mind JoseDokumen4 halamanPsychosomatic Means Mind JoseGopi KrishnanBelum ada peringkat
- 6 Construction of ShoeDokumen33 halaman6 Construction of ShoevedBelum ada peringkat
- When - Walking.fails - Ebook DDUDokumen384 halamanWhen - Walking.fails - Ebook DDURajeev GulrajaniBelum ada peringkat
- Back To The Basics of SpeedDokumen20 halamanBack To The Basics of SpeedBukan PujanggaBelum ada peringkat
- Assisting With Walking Using Walker and Cane, CrutchesDokumen26 halamanAssisting With Walking Using Walker and Cane, CrutchesIbrahim R. Ayasreh100% (1)
- Pedestrians FirstDokumen73 halamanPedestrians FirstDisability Rights AllianceBelum ada peringkat
- A Backward Walking Training Program To ImproveDokumen10 halamanA Backward Walking Training Program To ImproveRadhiatul AdillahBelum ada peringkat
- Alterations in Gait Velocity and Grip Strength of Stroke Survivors Following A 12-Week Structured Therapeutic Exercise ProgrammeDokumen5 halamanAlterations in Gait Velocity and Grip Strength of Stroke Survivors Following A 12-Week Structured Therapeutic Exercise ProgrammeCristina MuyargasBelum ada peringkat
- Gaitan 1 PDFDokumen12 halamanGaitan 1 PDFDeborah SalinasBelum ada peringkat
- Validation of The Godin Leisure-Time Exercise Questionnaire Class PDFDokumen11 halamanValidation of The Godin Leisure-Time Exercise Questionnaire Class PDFKishenthi KerisnanBelum ada peringkat
- Effects of Aerobic Exercise Using Cycle Ergometry On Balance and Functional Capacity in Post Stroke Patients A Systematic Review and Meta AnalysisDokumen8 halamanEffects of Aerobic Exercise Using Cycle Ergometry On Balance and Functional Capacity in Post Stroke Patients A Systematic Review and Meta Analysisluigi.adacampoBelum ada peringkat
- A Systematic Review of Mechanisms of Gait Speed Change Post-Stroke. Part 1... Spatiotemporal Parameters and Asymmetry RatiosDokumen13 halamanA Systematic Review of Mechanisms of Gait Speed Change Post-Stroke. Part 1... Spatiotemporal Parameters and Asymmetry RatiosJohann Sebastian CruzBelum ada peringkat
- Bean 2010Dokumen6 halamanBean 2010壮Belum ada peringkat
- Effects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisDokumen12 halamanEffects of Exercise On Quality of Life in Stroke Survivors: A Meta-AnalysisNoor KameliaBelum ada peringkat
- ProQuestDocuments 2017 11 11 PDFDokumen13 halamanProQuestDocuments 2017 11 11 PDFDonny HendrawanBelum ada peringkat
- Lifestyle ModiwcationsDokumen2 halamanLifestyle ModiwcationsGeorge RulesBelum ada peringkat
- Literature Review Cardiac RehabilitationDokumen5 halamanLiterature Review Cardiac Rehabilitationafmzitaaoxahvp100% (1)
- Hop Testing Provides A Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction PDFDokumen13 halamanHop Testing Provides A Reliable and Valid Outcome Measure During Rehabilitation After Anterior Cruciate Ligament Reconstruction PDFCleber PimentaBelum ada peringkat
- Intra Dial y TicDokumen8 halamanIntra Dial y Ticratna220693Belum ada peringkat
- AHA Heart Article 2 Week 13Dokumen12 halamanAHA Heart Article 2 Week 13beniak_preBelum ada peringkat
- Accepted: Mechanisms For Improved Running Economy in Beginner RunnersDokumen27 halamanAccepted: Mechanisms For Improved Running Economy in Beginner RunnersmadloloBelum ada peringkat
- Actividad Fisica 2016Dokumen18 halamanActividad Fisica 2016Omar DVBelum ada peringkat
- Hydrotherapy Vs Gym Exercises For OADokumen7 halamanHydrotherapy Vs Gym Exercises For OAketchitoBelum ada peringkat
- Importante Protocolo de Ejercicios en PiscinaDokumen14 halamanImportante Protocolo de Ejercicios en PiscinaEduardo Santana SuárezBelum ada peringkat
- Main 27Dokumen16 halamanMain 27pokharelriwaj82Belum ada peringkat
- Functional Electrical Stimulation With Exercises For Standing Balance and Weight Transfer in Acute Stroke PatientsDokumen9 halamanFunctional Electrical Stimulation With Exercises For Standing Balance and Weight Transfer in Acute Stroke PatientsAugusto ManoelBelum ada peringkat
- Ijspt 14 564Dokumen18 halamanIjspt 14 564WaterfloBelum ada peringkat
- v062p01162 PDFDokumen6 halamanv062p01162 PDFPilar Riquelme AguilarBelum ada peringkat
- There Is No Superior Treatment in Improving Gait in Patients With Chronic StrokeDokumen6 halamanThere Is No Superior Treatment in Improving Gait in Patients With Chronic Strokerc_delarosa5767Belum ada peringkat
- Balance TrainingDokumen12 halamanBalance TrainingMahdicheraghi100% (1)
- Treino de ResisteenciaDokumen10 halamanTreino de ResisteenciaJosé Ricardo Martins JuniorBelum ada peringkat
- 2015 Article 155Dokumen16 halaman2015 Article 155Tito AlhoBelum ada peringkat
- Sullivan Et Al 2007 STEPS-CR 5Dokumen23 halamanSullivan Et Al 2007 STEPS-CR 5Karen PohlBelum ada peringkat
- An Intensive Virtual Reality Program Improves Functional Balance and Mobility of Adolescents With Cerebral PalsyDokumen9 halamanAn Intensive Virtual Reality Program Improves Functional Balance and Mobility of Adolescents With Cerebral PalsyStephGrenBelum ada peringkat
- Efectos Del Ejercicio en Pacientes Mayores Con Diabetes ECADokumen13 halamanEfectos Del Ejercicio en Pacientes Mayores Con Diabetes ECAAndrés Araneda VásquezBelum ada peringkat
- Art - Equilibrio y PropiocepcionDokumen7 halamanArt - Equilibrio y PropiocepcionYuLyChBelum ada peringkat
- Joi 160003Dokumen11 halamanJoi 160003api-292843843Belum ada peringkat
- Research in Sports Medicine: An International JournalDokumen18 halamanResearch in Sports Medicine: An International JournalCleber PimentaBelum ada peringkat
- The Effects of Cycling With and WithoutDokumen24 halamanThe Effects of Cycling With and WithoutdanielBelum ada peringkat
- Neuromuscular Training Improves Single-Limb Stability in Young Female AthletesDokumen12 halamanNeuromuscular Training Improves Single-Limb Stability in Young Female AthletesyarnlarbizimdirBelum ada peringkat
- Medicina 55 00726 v3Dokumen21 halamanMedicina 55 00726 v3Consulta Médica AriasBelum ada peringkat
- RevisionSistematicayMetaanalisis - TFNP.Stroke MariaJulianaGonzalezSilva ArticuloDokumen18 halamanRevisionSistematicayMetaanalisis - TFNP.Stroke MariaJulianaGonzalezSilva Articulomariasol63Belum ada peringkat
- Ultrasound Assessment of Trunk Muscles and Back Flexibility, Strength and Endurance in Off-Road Cyclists With and Without Low Back PainDokumen10 halamanUltrasound Assessment of Trunk Muscles and Back Flexibility, Strength and Endurance in Off-Road Cyclists With and Without Low Back PainSebastian EderBelum ada peringkat
- Rehabilitation AmbulationDokumen14 halamanRehabilitation AmbulationDeborah SalinasBelum ada peringkat
- The Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisDokumen20 halamanThe Effectiveness of Physiotherapy Exercises in Subacromial Impingement Syndrome: A Systematic Review and Meta-AnalysisBruno FellipeBelum ada peringkat
- Otago Home-Based Strength and Balance Retraining Improves Executive Functioning in Older Fallers - A Randomized Controlled Trial.Dokumen10 halamanOtago Home-Based Strength and Balance Retraining Improves Executive Functioning in Older Fallers - A Randomized Controlled Trial.Ed RibeiroBelum ada peringkat
- Effectiveness of Physiotherapy Exercise After Knee Arthroplasty For OsteoarthritisDokumen2 halamanEffectiveness of Physiotherapy Exercise After Knee Arthroplasty For OsteoarthritisGopi KrishnanBelum ada peringkat
- Arm 41 34Dokumen8 halamanArm 41 34pashaBelum ada peringkat
- Effetti Delle Tem e Della Mobilizzazione Articolare Su Spalla Di Giovani Sportivi Overhead LanciatoriDokumen8 halamanEffetti Delle Tem e Della Mobilizzazione Articolare Su Spalla Di Giovani Sportivi Overhead LanciatoriTommaso BusilacchiBelum ada peringkat
- Educating Patients About The Benefits of Physical Activty and Exercise For Their Hip and Knee OA SDokumen10 halamanEducating Patients About The Benefits of Physical Activty and Exercise For Their Hip and Knee OA SjotaBelum ada peringkat
- 55.literature Review About Neurodevelopmental Approaches-1Dokumen37 halaman55.literature Review About Neurodevelopmental Approaches-1Zeeshan AhmadBelum ada peringkat
- Motor Control Exercise For Persistent, Nonspecific Low Back Pain: A Systematic ReviewDokumen17 halamanMotor Control Exercise For Persistent, Nonspecific Low Back Pain: A Systematic ReviewPethuel PomaloyBelum ada peringkat
- FitnessDokumen32 halamanFitnessFernanda LopezBelum ada peringkat
- CRP2020 1236968Dokumen9 halamanCRP2020 1236968Lal NandaniBelum ada peringkat
- Cambios en Dorsiflexión y Control Postural Dinámico Tras Movilizaciones en Individuos Con Inestabilidad Crónica Del TobilloDokumen15 halamanCambios en Dorsiflexión y Control Postural Dinámico Tras Movilizaciones en Individuos Con Inestabilidad Crónica Del Tobillocontact.movementsiteBelum ada peringkat
- Relative Intensity of Physical Activity and Risk of Coronary Heart DiseaseDokumen17 halamanRelative Intensity of Physical Activity and Risk of Coronary Heart DiseaseWidya SyahdilaBelum ada peringkat
- Cherng Et Al. (2007)Dokumen8 halamanCherng Et Al. (2007)ع الBelum ada peringkat
- Kabat 4Dokumen19 halamanKabat 4Nathalia Gutierrez RestrepoBelum ada peringkat
- Fundamental Movement and DynamicDokumen9 halamanFundamental Movement and DynamicYoh ChenBelum ada peringkat
- DONEDokumen7 halamanDONEpashaBelum ada peringkat
- 10.1093 PTJ Pzac153Dokumen13 halaman10.1093 PTJ Pzac153evelyn.minichBelum ada peringkat
- 2016 Article 206Dokumen10 halaman2016 Article 206Rinto Sapta Andreas SimanjuntakBelum ada peringkat
- ProQuestDocuments 2014-11-12Dokumen12 halamanProQuestDocuments 2014-11-12shiddiqohajeBelum ada peringkat
- Body Weight Changes and Corresponding Changes in Pain and Function in Persons With Symptomatic Knee Osteoarthritis: A Cohort StudyDokumen8 halamanBody Weight Changes and Corresponding Changes in Pain and Function in Persons With Symptomatic Knee Osteoarthritis: A Cohort StudyMiguelBelum ada peringkat
- Protocolo Fuerza HandgripDokumen5 halamanProtocolo Fuerza HandgripValeria Tabares SanchezBelum ada peringkat
- Exercise Physiology for the Pediatric and Congenital CardiologistDari EverandExercise Physiology for the Pediatric and Congenital CardiologistBelum ada peringkat
- Muscle Energy Technique: Active Knee Extension Test Muscle Energy Technique Mean Difference T Value DF SignificantDokumen7 halamanMuscle Energy Technique: Active Knee Extension Test Muscle Energy Technique Mean Difference T Value DF SignificantGopi KrishnanBelum ada peringkat
- Chest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryDokumen5 halamanChest Physiotherapy or Techniques in Cardio Pulmonary Physiotherapy A Running CommentaryGopi KrishnanBelum ada peringkat
- Acknowledgement: and Sports Medicine), Vice Principal, Bethany Navajeevan College of Physiotherapy, For HerDokumen1 halamanAcknowledgement: and Sports Medicine), Vice Principal, Bethany Navajeevan College of Physiotherapy, For HerGopi KrishnanBelum ada peringkat
- GOPIKRISHNANDokumen1 halamanGOPIKRISHNANGopi KrishnanBelum ada peringkat
- Gopikrishnan.C.G: Career ObjectiveDokumen4 halamanGopikrishnan.C.G: Career ObjectiveGopi KrishnanBelum ada peringkat
- Background and ObjectivesDokumen2 halamanBackground and ObjectivesGopi KrishnanBelum ada peringkat
- Name: Age: Sex: Date:: Data Collection SheetDokumen1 halamanName: Age: Sex: Date:: Data Collection SheetGopi KrishnanBelum ada peringkat
- Posterior Cruciate Ligament InjuriesDokumen26 halamanPosterior Cruciate Ligament InjuriesGopi KrishnanBelum ada peringkat
- Gopi KrishnanDokumen1 halamanGopi KrishnanGopi KrishnanBelum ada peringkat
- Physiotherapy in Orthopeadic ConditionsDokumen2 halamanPhysiotherapy in Orthopeadic ConditionsGopi KrishnanBelum ada peringkat
- Instructions For Six Minute Walk Test Form SMW, Version 1.0 (QXQ)Dokumen4 halamanInstructions For Six Minute Walk Test Form SMW, Version 1.0 (QXQ)Gopi KrishnanBelum ada peringkat
- Comparison Between Task Oriented Training and Proprioceptiveneuromuscular Facilitation Exercises On Lower Extremity Function Ince 2165 7025 1000291Dokumen9 halamanComparison Between Task Oriented Training and Proprioceptiveneuromuscular Facilitation Exercises On Lower Extremity Function Ince 2165 7025 1000291Gopi KrishnanBelum ada peringkat
- Veverka Planning Interpretive WalkingtoursDokumen9 halamanVeverka Planning Interpretive WalkingtoursLeOn Wzz 众Belum ada peringkat
- CM AW15 Brochure Web PricedDokumen72 halamanCM AW15 Brochure Web PricedromyluleBelum ada peringkat
- Biomecanica Da ObesidadeDokumen9 halamanBiomecanica Da ObesidadehgtrainerBelum ada peringkat
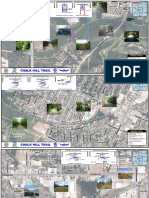
- Chalk Hill Trial MapsDokumen3 halamanChalk Hill Trial MapsRachel Yates StoneBelum ada peringkat
- Wakefield Countryside Directory For People With Disabilities PDFDokumen56 halamanWakefield Countryside Directory For People With Disabilities PDFJanBelum ada peringkat
- Bombay Hospital ProjectDokumen38 halamanBombay Hospital Projectprutha khadeBelum ada peringkat
- W. PA - Bavington Letter 2.0Dokumen1 halamanW. PA - Bavington Letter 2.0MikeBelum ada peringkat
- Gait Biomechanics 1Dokumen43 halamanGait Biomechanics 1Dibyendunarayan Bid50% (2)
- Foot Trajectory For A Quadruped Walking MachineDokumen8 halamanFoot Trajectory For A Quadruped Walking MachineMer FroBelum ada peringkat
- Ensino Médio Carnival Texto e InterpretaçãoDokumen3 halamanEnsino Médio Carnival Texto e InterpretaçãoJean de SousaBelum ada peringkat
- Splay Shoes Sizing Guide 3.1Dokumen1 halamanSplay Shoes Sizing Guide 3.1borja garcia sastreBelum ada peringkat
- Ladies - BRND Wise-19-20Dokumen440 halamanLadies - BRND Wise-19-20SatyaBelum ada peringkat
- Staircase II Full Tread BifurcatedDokumen1 halamanStaircase II Full Tread BifurcatedStuti ParikhBelum ada peringkat
- Easy Shoe Size Conversion Charts US UK EURODokumen1 halamanEasy Shoe Size Conversion Charts US UK EUROkaiBelum ada peringkat
- Return DemonstrationDokumen8 halamanReturn DemonstrationCDT Feliciano Fernando JardelezaBelum ada peringkat
- Explore The Dallas-Fort Worth VelowebDokumen2 halamanExplore The Dallas-Fort Worth VelowebKERANewsBelum ada peringkat
- Exo MITDokumen139 halamanExo MITAautresBelum ada peringkat
- September 2014 Trinity TrumpetDokumen18 halamanSeptember 2014 Trinity TrumpetTrinityUMCBelum ada peringkat
- BioMechanic Lab Study of The Gait KinematicsDokumen5 halamanBioMechanic Lab Study of The Gait Kinematicsعباس حماديBelum ada peringkat
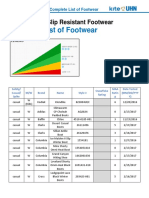
- Complete - List - of - Footwear - Tested - Nov - 11 - 2022Dokumen18 halamanComplete - List - of - Footwear - Tested - Nov - 11 - 2022Dado TorcisoBelum ada peringkat
- Asimo Technical FaqDokumen8 halamanAsimo Technical FaqEko PrasBelum ada peringkat
- Assignment-10question and SolutionDokumen21 halamanAssignment-10question and SolutionshardasiddhBelum ada peringkat