Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Mastering Your Adult ADHD A Cognitive Behavioral Treatment ProgramDokumen145 halamanMastering Your Adult ADHD A Cognitive Behavioral Treatment ProgramLilia Botnaru96% (28)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Risk Assessment in PsychiatryDokumen56 halamanRisk Assessment in PsychiatryAmin ZahariBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Filaria - A Comprehensive StudyDokumen63 halamanFilaria - A Comprehensive StudyDayledaniel SorvetoBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- McDonald John - Chinese Versus French Perspectives On The Channel SystemDokumen17 halamanMcDonald John - Chinese Versus French Perspectives On The Channel SystemAssaf FeldmanBelum ada peringkat
- CholilithiasisDokumen94 halamanCholilithiasisdr.hendraBelum ada peringkat
- Nursing Care PlansDokumen16 halamanNursing Care PlansSantos Kyla Patricia T.Belum ada peringkat
- نسخة Lecture - PAIN Assessment & ManagementDokumen52 halamanنسخة Lecture - PAIN Assessment & Managementjsoal100% (1)
- Implant Dentistry - A Rapidly Evolving PracticeDokumen556 halamanImplant Dentistry - A Rapidly Evolving Practicedrescobedocomf67% (3)
- Drug Used in The Therapy of Shock.Dokumen8 halamanDrug Used in The Therapy of Shock.Vennela100% (1)
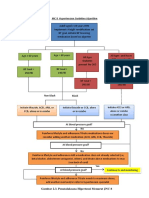
- Algoritma Tatalaksana HTDokumen2 halamanAlgoritma Tatalaksana HTUswatun Hasanah RIBelum ada peringkat
- Eff Pleura & PneumothoraxDokumen69 halamanEff Pleura & PneumothoraxUswatun Hasanah RIBelum ada peringkat
- Lamp IranDokumen5 halamanLamp IranUswatun Hasanah RIBelum ada peringkat
- ReferensiDokumen2 halamanReferensiUswatun Hasanah RIBelum ada peringkat
- Cuidados Diabetes 2016Dokumen119 halamanCuidados Diabetes 2016Diego Pizarro ReyesBelum ada peringkat
- Kulpend Infeksi Imuno - RevisiDokumen44 halamanKulpend Infeksi Imuno - RevisiUswatun Hasanah RIBelum ada peringkat
- PhenylketonuriaDokumen8 halamanPhenylketonuriaAmberlee PetiBelum ada peringkat
- Miyagawa Et Al-2015-Human Genome VariationDokumen4 halamanMiyagawa Et Al-2015-Human Genome Variationece142Belum ada peringkat
- Bachelor of Science in Project and Facility Management With Honours MAY 2020Dokumen17 halamanBachelor of Science in Project and Facility Management With Honours MAY 2020Suziah Baindis AngkimBelum ada peringkat
- Module 25 Hospital Hygiene Infection Control and HCWM - EnglishDokumen38 halamanModule 25 Hospital Hygiene Infection Control and HCWM - Englishkhuzaima9Belum ada peringkat
- (MRSA) InfectionDokumen21 halaman(MRSA) InfectionKhurram NadeemBelum ada peringkat
- ECR 2022 ProgrammeDokumen1.126 halamanECR 2022 ProgrammejbmbritoBelum ada peringkat
- PMLS (Mod 1-3)Dokumen23 halamanPMLS (Mod 1-3)Ja NaeBelum ada peringkat
- Savita S. Angadi - 8163Dokumen4 halamanSavita S. Angadi - 8163Vishal BantiBelum ada peringkat
- FIQ - Proliferative Diabetic RetinopathyDokumen35 halamanFIQ - Proliferative Diabetic RetinopathyHikban FiqhiBelum ada peringkat
- Upload 29Dokumen4 halamanUpload 29Lenny SilalahiBelum ada peringkat
- Factors Affecting Stability of OrthodontDokumen7 halamanFactors Affecting Stability of OrthodontSALAHEDDINE BLIZAKBelum ada peringkat
- Myocardial Infarction: Classification of ACSDokumen7 halamanMyocardial Infarction: Classification of ACSMaria Charis Anne IndananBelum ada peringkat
- Shoulder Problems / Shoulder Injuries in RugbyDokumen10 halamanShoulder Problems / Shoulder Injuries in RugbyAvinash NithyanandBelum ada peringkat
- M3 Health HomeworkDokumen1 halamanM3 Health HomeworkKarlyBelum ada peringkat
- ANTIJAMURDokumen3 halamanANTIJAMURCharlesMahonoBelum ada peringkat
- UELS NIH Research Plan CompressedDokumen36 halamanUELS NIH Research Plan CompressedKunal JaisinghaniBelum ada peringkat
- TULUA Lipoabdominoplasty Transversal Aponeurotic.12Dokumen14 halamanTULUA Lipoabdominoplasty Transversal Aponeurotic.12Carolina Ormaza Giraldo100% (1)
- Kibi - DSTC - How To Keep The PT Alive I Juni 21Dokumen32 halamanKibi - DSTC - How To Keep The PT Alive I Juni 21tepat rshsBelum ada peringkat
- Albert Et Al. The Efficacy of Systematic Active Conservative Treatment For Patients With Severe Sciatica - AbstractDokumen2 halamanAlbert Et Al. The Efficacy of Systematic Active Conservative Treatment For Patients With Severe Sciatica - AbstractPremanandi Devi DasiBelum ada peringkat
- Public Health NutritionDokumen58 halamanPublic Health NutritionJaime TaylorBelum ada peringkat
- Introduction To Nicotine and Caffeine AddictionDokumen10 halamanIntroduction To Nicotine and Caffeine AddictionUltra BlochBelum ada peringkat